Introduction
Gastrointestinal lipomas are uncommon benign tumours that occur anywhere along the gut. The most common location for these lesions is the colon, followed by the ileum and the jejunum. Lipomas found in the duodenum {Duodenal Lipomas (DLs)} are very rare with limited case reports present in literature. When small, DLs are often discovered incidentally at laparotomy [1-4]; when larger, they can manifest through acute lesions of the overlying mucosa or the gastrointestinal wall, for example, ulceration [5] or gastrointestinal bleeding [6,7], abdominal pains, intussusceptions [8] or intestinal obstruction [2,9]. Owing to recent advances in endoscopy and modern imaging techniques such as CT scan and MRI, more cases are being diagnosed and treated. However, no systematic study of DLs has been reported. This review focuses on a retrospective analysis of a series of 59 patients with DL, summarize the clinical presentation, diagnosis and treatment of DL.
Case Report
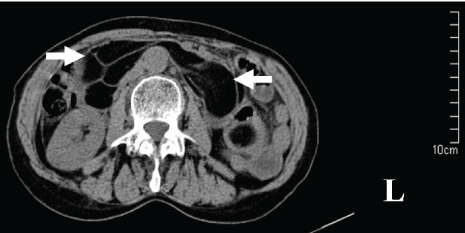
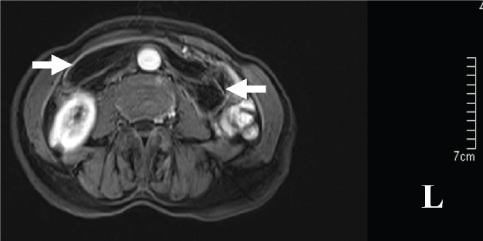
A 67-year-old woman was transferred to our hospital with one-day history of abdominal pain, vomit and constipation. She had a five years history of epigastric fullness and intermittent, upper abdominal pain in the past. CT revealed intestinal obstruction and hypodense lesions with CT value of -64 housefield units (HU) to -138 HU located from the descending part of the duodenum to the proximal jejunum, which was suggestive of lipomas [Table/Fig-1]. MR showed fat-containing mass lesions and the masses were high-intensity on T1-weighted and intermediately intensity on T2-weighted images [Table/Fig-2], with a drop in signal on T1 and T2-weighted fat-suppressed images [Table/Fig-3], consistent with a diagnosis of duodenal lipomas.
CT scan appearance of duodenal lipoma.
Axial T1-weighted MRI shows a well-demarcated, hyperintense mass (arrow).

MRI showing the lesions drop in signal on T1 -weighted fat-suppressed image.
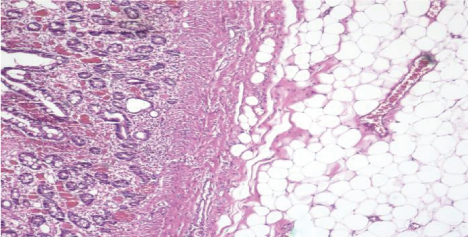
The patient then underwent exploratory laparotomy and multiple, giant lipomas could be palpated in second, third, fourth part of duodenum and proximal jejunum. Duodenum 4 cm distal to ampulla was excised along with 14 cm of proximal jejunum [Table/Fig-4]. Intestinal continuity was maintained by end-to-end duodenojejunal hand-sewn anastomosis. The postoperative period was uncomplicated and she was discharged from the hospital successfully. Final histopathological diagnosis of the specimen were multiple, submucosal lipomas vary from 1.3 × 1.3 × 1.0 cm to 11.0 × 5.0 × 4.0 cm [Table/Fig-5].
Excised submucous, multiple lipomatosis showing naked fat sign.

Pathological report indicating duodenal lipoma originating in submucosal layer (H&E 4x).
Materials and Methods
A systematic literature search was performed using the PubMed database (from 1948 to December 2016) by using the keyword “duodenal lipoma”. The search terms were found in the abstract, title or medical subject heading. Excluded from this review were review articles, expert opinions and studies that were published in languages other than English. The articles that were generated in each step of the search were then aggregated to produce an article list for consideration. Two reviewers independently screened the article titles, abstracts and full texts for further analysis [Table/Fig-6]. Data extracted from each paper included age, sex, number of the lipoma, maximum dimension of the mass, presentation, location, pattern of growth, imaging features, diagnosis and therapy.
Flow diagram of article selection for inclusion in this study.
(on initial assessment all abstracts were in English but in six articles the full text was found to be in non-English).

Results
Using the search strategy listed above, 218 articles were identified. [Table/Fig-6] shows the flowchart of the inclusion and exclusion of the potential studies. During the review of the title, abstract and full text, an additional 166 articles were excluded, resulting in 52 articles that were finally included in this systematic review. Of these 52 articles [3,4,6,7,9-56], there were 59 cases of DL so far reported in English. Of which 49 cases were solitary, 10 cases were multiple. Details of multiple DLs were shown in [Table/Fig-7]. Median age of presentation was 57-year-old (range 12 to 83) with female to male ratio of 30:29. The age onset is shown in [Table/Fig-8]. The maximum diameter of the tumours ranged from 0.6 cm to 11 cm (mean diameter 4.1 cm). The location distribution of the tumour was shown in [Table/Fig-9]. The pattern of growth was mucosal in four cases, submucosal in forty-five and subserosal in one case. DL may present with obstruction, bleeding, dyspepsia, epigastric pain and discomfort. The diagnostic accuracy of CT, MRI, EUS, endoscopy and biopsy was shown in [Table/Fig-10]. The treatments include observation, endoscopic excision or surgery which was shown in [Table/Fig-11].
Summary of case reports of multiple duodenal lipomas from 1948 to 2016 [10-19].
| Reference | Age, sex | Presentation | Location | Maximum dimension in cm | Number | Treatment |
|---|
| 1. Fawcett NW et al., [10] | 36, M | Melena, fatigue, abdominal discomfort, nausea | D2 | 7 | 2 | Partial duodenectomy |
| 2. Kirkland WG and Boyer RA [11] | 60, F | Abdominal pain, vomit | D2 | 7 | 3 | Transduodenal resection cholecystectomy T-tube was inserted into the common duct |
| 3. Deeths TM et al., [12] | 50, F | Epigastric discomfort, vomit | G, D | - | Multiple | Duodenotomy and mass excision |
| 4. Devlies F et al., [13] | 67, F | Asymptomatic | G, D1, D2 | - | Multiple | Endoscopic biopsy |
| 5. Lundell L et al., [14] | 44, M | Obstructive jaundice, gastricoutlet obstruction | D2, D3, D4 | - | Multiple | Pancreas-sparing duodenectomy |
| 6. Liu X et al., [15] | 36, M | Asymptomatic | D | - | Multiple | - |
| 7. Kovač JD et al., [16] | 65, M | Postprandial fullness, vomit, epigastric pain | D1, D2 | 2.5 | 3 | Surgery |
| 8. Weinstock LB et al., [17] | 56, M | Asymptomatic | D1, D2, D3 | 2 | Multiple | Biospy |
| 9. Jayasundara J et al., [18] | 43, F | Constipation, vomit | D2, D3, D4, J | - | Multiple | Bypass |
| 10. Zirpe D et al., [19] | 45, M | Melena | D2, D3, D4, J | 4 | 4 | Duodenectomy (D3,D4) |
| 11. Present case | 67, F | Abdominal pain, vomit, constipation | D2, D3, D4, J | 11 | 21 | Duodenectomy |
F= Female, M= Male, D= Duodenum, G= Gastric, J= Jejunum
Age distribution of patients with duodenal lipoma.

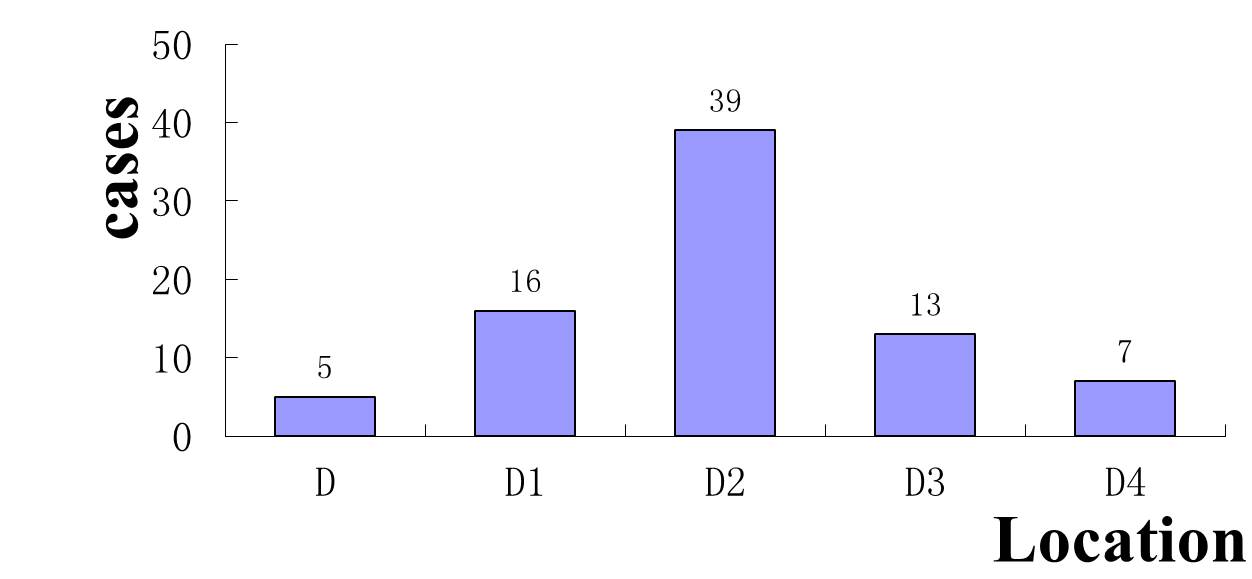
Location distribution of the tumour.
The diagnostic accuracy of each method.

Summary of the treatment.

Discussion
DLs are extremely rare. Indeed, the incidence of DL is only limited to case report. The DLs are benign and slow growing tumours. Malignant change is unheard of with these lesions [9]. The peak of incidence seems to be around the fifth and seventh decade of life which can be seen in [Table/Fig-8]. The exact aetiology of DL remains unknown. It might be associated with embryonic displacement of adipose tissue, degenerative disease with disturbance of fat metabolism [57] or dyslipidemia [24].
According to our study, as shown in [Table/Fig-9], lipomas tend to be noted mostly in the second part of the duodenum. The majority of the DLs arise from the submucosa [3,4] but may extend through the bowel wall and into the serosal or mesenteric fat. DL presents as a round or ovoid, soft mass with regular or lobulated contours. They can be either sessile or pedunculate. The overlying mucosa of the duodenal lipoma is usually normal, but there may be areas of ulceration or erosion. Multiple DL is very rare, there is only 11 cases reported so far including our case.
The clinical symptoms of DL are always non-special for an early diagnosis, with vague abdominal complaints common in the general population that is often dismissed initially by the consulted physician. Their rarity and failure to consider the disease often lead to a late evaluation of an advanced state of disease at diagnosis. Some patients usually have had symptoms for several months prior to diagnosis. Most of the DLs remain asymptomatic and are discovered incidentally during endoscopy, surgery [3,4,6,41] or autopsy. Symptoms are related to the characteristic of the lipoma, such as size and location. According to our survey, 80% of symptomatic DLs are larger than 2 cm in diameter. If symptomatic, the most common clinical presentation is that of epigastric fullness gradually becoming worse and leading to obstruction [9,58], bleeding [6,7] due to the stretching of the mucosa, with necrosis of the overlying epithelial layers [19], intussusceptions [8] that is rare due to the relatively fixed anatomical position of the duodenum, painless obstructive jaundice and finally pancreatitis. The case with pancreatitis reported by McGrath FP et al., is particularly unusual [26]. The symptoms of DL are nonspecific and hence, they are not useful for differential diagnosis.
Because early symptoms are often nonspecific and vague, it is important to keep the diagnosis of DL in the differential diagnosis of obscure abdominal pain or gastrointestinal tract bleeding. Despite consideration of this diagnosis, it can still be difficult to confirm. Diagnosis can be established by radiological, endoscopic or operative means. Current imaging modalities, such as CT and MRI can provide an accurate diagnosis [16]. DLs appear on CT as a well-circumscribed hypodense lesion with a density ranging from -60 to -120 HU [59]. As fat suppression techniques effectively reduce the macroscopic fat signal, they are preferred in order to diagnose lipomas with MR [16]. Lipomas have high-intensity on T1-weighted images and usually present intermediate intensity on T2-weighted images. The loss of signal on fat-suppressed images enables the final diagnosis by MRI [16]. Though CT and MRI are helpful in diagnosis but these are unable to precisely locate the origin of the lesion. Direct visualization at endoscopy provides the clues about the nature of the tumour. In most cases, endoscopy has become the choice for diagnosis, either by the appearance of a pedunculate mass of fat or of a lesion stretching the sub-mucosa and when the mucosa is uncovered the shiny yellow colour of the lipoma becomes apparent “the naked fat sign” [44]. But it is generally insufficient in making a definitive diagnosis by endoscopy if the lipoma is submucosal or subserol. EUS is effective to provide information about the original layer, echogenicity, the depth and invasion [34]. The typical EUS findings for DLs are intense homogeneous hyperechoic mass originating from the submucosa, with echo attenuation behind and/or inside the rear area [58]. If the lipoma is within reach of the endoscope, a biopsy forcep can be used to prove the diagnosis. Before biopsy of the putative lipoma, however, the diagnosis might be suspected. The “naked fat sign”, “pillow sign” and “tenting sign” [17] have been said to be pathognomonic.
The asymptomatic DL can be observed, but symptomatic DL needs treatment. It can be excised endoscopically or operatively. The pedunculated, small, solitary lipoma can be easily and safely removed by either “snare” polypectomy or “endoloop” [3,4,7]. For large and sessile lesions, endoscopic excision may prove technically difficult and increase the risk of bleeding and perforation [60]. These types of lipomas are difficult to manage using endoscopic techniques, thus surgical excision would be the preferred approach. If the nature of the lesion cannot be ascertained or clinical presentation such as intussusception, surgery is required. Operative management is mainly divided into four procedures, excision of the lipoma via a duodenotomy [11,12,16,23,26], segment bowel resection [20], PSD [14] or bypass [18,32]. The type of procedure chosen to perform depends on the patient’s condition as well as the size and position of the tumour. The localization of the tumour is the key step and can be done by intraoperative endoscopy, where endoscopic transillumination aids in locating the exact site of the lesion or in identifying the “naked fat sign” [23] when the lipoma is subserosal. Most of the cases are managed by opening the duodenum and resected the mass according to our review. For periampullary neoplasms, local resection of the tumour with plastic repair of Oddi sphincter or pancreatoduodenectomy is recommended. Pancreas-sparing duodenectomy was performed in one case because the lipomas invaginated into the duodenojejunal flexure and the patient had a history of obstructive jaundice [20]. However, the standard pancreatoduodenectomy is not suitable for DL unless the ampullary carcinoma coexists. Gastrostomy, jejunostomy with a T-tube stented the common duct is recommended to prevent the anastomotic leakage. In case the excision of the entire duodenum is not safe, a bypass to the lesion is recommended [18]. Laparoscopy has been recently described for the management of DL, which is a minimally invasive mode of surgical management with minimal postoperative pain and short hospitalization [28,44]. Robotic technology has been shown the technical advantages to facilitate complex resection and reconstruction during periampullary procedures [61].
Conclusion
DL is a rare kind of gastrointestinal tumour. Patients may be asymptomatic or present with gastrointestinal bleeding, intussusceptions or bowel obstruction. The successful diagnostic means are CT, MRI, endoscopy and EUS. Many of these lesions require surgical resection as a result of their size and location. Since, DL is a kind of benign tumour, it might be more desirable to employ the less invasive endoscopic excision or laparoscopy excision whenever this is possible.
F= Female, M= Male, D= Duodenum, G= Gastric, J= Jejunum
[1]. O’Riordan BG, Vilor M, Herrera L, Small bowel tumours: an overviewDig Dis 1996 14(4):245-57. [Google Scholar]
[2]. Lee KJ, Kim GH, Park DY, Shin NR, Lee BE, Ryu DY, Endoscopic resection of gastrointestinal lipomas: a single-center experienceSurg Endosc 2014 28(1):185-92. [Google Scholar]
[3]. In Ho J, Young Hee M, Safe techniques for endoscopic resection of gastrointestinal lipomasGastric Cancer 2010 10(4):254-58. [Google Scholar]
[4]. Tsou YK, Liu NJ, Jan YY, Biliary obstruction caused by hemobilia after endoscopic sphincterotomy in a patient with an anomalous location of papilla of VaterGastrointest Endosc 2008 68(6):1232-34. [Google Scholar]
[5]. Zirpe D, Wani M, Tiwari P, Ramaswamy PK, Kumar RP, Duodenal lipomatosis as a curious cause of upper gastrointestinal bleed: a report with review of literatureJ Clin Diagn Res 2016 10(5):PE01-PE4. [Google Scholar]
[6]. Kadaba R, Bowers KA, Wijesuriya N, Preston SL, Bray GB, Kocher HM, An unusual cause of gastrointestinal bleeding: duodenal lipomaCase Rep Gastroenterol 2011 5(1):183-88. [Google Scholar]
[7]. Tung CF, Chow WK, Peng YC, Chen GH, Yang DY, Kwan PC, Bleeding duodenal lipoma successfully treated with endoscopic polypectomyGastrointest Endosc 2001 54(1):116-17. [Google Scholar]
[8]. Knight CD, Black BM, Duodenojejunal intussusception due to lipoma: report of a caseProc Staff Meet Mayo Clin 1951 26:320-23. [Google Scholar]
[9]. Blanchet MC, Arnal E, Paparel P, Grima F, Voiglio EJ, Caillot JL, Obstructive duodenal lipoma successfully treated by endoscopic polypectomyGastrointest Endosc 2003 58(6):938-39. [Google Scholar]
[10]. Fawcett NW, Bolton VL, Geever EF, Multiple lipomas of the stomach and duodenumAnn Surg 1949 129(4):524-27. [Google Scholar]
[11]. Kirkland WG, Boyer RA, Multiple lipomas of the duodenum:a case reportGastroenterology Res 1951 19(1):142-47. [Google Scholar]
[12]. Deeths TM, Madden PN, Dodds WJ, Multiple lipomas of the stomach and duodenumAm J Dig Dis 1975 20(8):771-74. [Google Scholar]
[13]. Devlies F, Van HL, Leemans AM, Ponette E, Paepe ID, Gastroduodenal lipomatosisEur Radiol 1997 7(3):338-40. [Google Scholar]
[14]. Lundell L, Hyltander A, Liedman B, Pancreas-sparing duodenectomy: technique and indicationsEur J Surg 2002 168(2):74-77. [Google Scholar]
[15]. Liu X, Wilcox CM, Nodit L, Audrey J, Lazenby Multiple gastrointestinal stromal tumours and lipomatosisArch Pathol Lab Med 2008 132(11):1125-29. [Google Scholar]
[16]. Kovac JD, Dunjic MK, Bjelovic M, Banko B, Lilic G, Milenkovic R, Magnetic resonance imaging features of multiple duodenal lipomas: a rare cause of intestinal obstructionJpn J Radiol 2012 30(8):676-79. [Google Scholar]
[17]. Weinstock LB, Axelbaum J, Norman E, Duodenal lipomatosisGastrointest Endosc 2013 77(6):954 [Google Scholar]
[18]. Jayasundara J, Sellahewa CS, Hall AD, Patel RT, A case of gastroduodenal lipomatosisAnn R Coll Surg Engl 2016 98(8):e203-e5. [Google Scholar]
[19]. Zirpe D, Wani M, Tiwari P, Ramaswamy PK, Kumar RP, Duodenal lipomatosis as a curious cause of upper gastrointestinal bleed: a report with review of literatureJ Clin Diagn Res 2016 10(5):PE01-PE4. [Google Scholar]
[20]. Spalding DR, Isla AM, Thompson JN, Williamson RC, Pancreas-sparing distal duodenectomy for infrapapillary neoplasmsAnn R Coll Surg Engl 2007 89(2):130-35. [Google Scholar]
[21]. Lee TH, Kim WJ, A duodenal lipoma with a long stalkKorean J Intern Med 2013 28(3):383 [Google Scholar]
[22]. Megibow AJ, Redmond PE, Bosniak MA, Horowitz L, Diagnosis of gastrointestinal lipomas by CTAJR Am J Roentgenol 1979 133(4):743-45. [Google Scholar]
[23]. Wichendu PN, Dodiyi-Manuel A, Gastric outlet obstruction from duodenal lipoma in an adultNiger J Surg 2013 19(2):79-81. [Google Scholar]
[24]. Bilgic Y, Altinsoy HB, Yildirim N, Alatas O, Kanat BH, Sahin A, Familial abdominal and intestinal lipomatosis presenting with upper GI bleedingCase Rep Gastrointest Med 2015 2015:123723 [Google Scholar]
[25]. Knoop RF, Richter-Schrag HJ, Walker C, Thimme R, Fischer A, Double-scope resection of a large duodenal polypEndoscopy 2015 47(Suppl 1):E627-28. [Google Scholar]
[26]. McGrath FP, Moote DJ, Langer JC, Orr W, Somers S, Duodenojejunal intussusception secondary to a duodenal lipoma presenting in a young boyPediatr Radiol 1991 21:590-91. [Google Scholar]
[27]. Michel LA, Ballet T, Collard JM, Bradpiece HA, Haot J, Severe bleeding from submucosal lipoma of the duodenumJ Clin Gastroenterol 1988 10(5):541-45. [Google Scholar]
[28]. Parmar AK, Bibyan M, Khandelwal R, Laparoscopic management of a large duodenal lipoma presented as gastric outlet obstructionJournal of the Society of Laparoendoscopic Surgeon 2013 17:459-62. [Google Scholar]
[29]. Krachman MS, Dave PB, Gumaste VV, Bleeding duodenal lipomaJ CIin Gustroenterol 1992 154(2):180-81. [Google Scholar]
[30]. Sou S, Nomura H, Takaki Y, Nagahama T, Matsubara F, Matsui T, Hemorrhagic duodenal lipoma managed by endoscopic resectionJ Gastroenterol Hepatol 2006 21(2):479-81. [Google Scholar]
[31]. Allison TD, Babcock JR, Lipoma of the duodenum causing melenaAnn Surg 1948 127(4):754-56. [Google Scholar]
[32]. Duthie HL, Forrest AP, Submucous lipoma of the duodenumBr J Surg 1957 45(190):201-02. [Google Scholar]
[33]. Mifuji-Moroka R, Iwasa M, Sugimoto R, Katsurahara M, Fujita N, Kobayashi Y, Education and imaging. Hepatobiliary and pancreatic: Liver abscess associated with lipoma of duodenumJ Gastroenterol Hepatol 2012 27(6):1129 [Google Scholar]
[34]. Malouf AJ, Patel RB, Sonographic appearance of a duodenal bulb lipoma with CT and MRI correlationJ Ultrasound Med 1991 10(8):461-64. [Google Scholar]
[35]. Efe C, Purnak T, Ozaslan E, Kucukciloglu Y, Which is the best approach for the hemorrhagic duodenal lipoma: endoscopic resection or surgery?Am J Surg 2012 203(4):558 [Google Scholar]
[36]. Cao D, Sun X, Du J, Sun Y, Duodenal lipoma associated with ectopic duodenal glandsClin Pract 2011 1(4):e128 [Google Scholar]
[37]. Murata A, Osoegawa T, Ijyu M, Kanayama K, Tanaka M, Nakamura K, Pedunculated duodenal lipoma treated with endoscopic polypectomy with a detachable snareFukuoka Igaku Zasshi 2008 99(6):131-35. [Google Scholar]
[38]. Jennings BS, Doerr RJ, Buffalo Duodenal lipoma causing intussusceptionSurgery 1989 105(4):560-63. [Google Scholar]
[39]. Lemer J, Haemorrhage from a polypoid lipoma of duodenumProc R Soc Med 1971 64(4):395 [Google Scholar]
[40]. Yaman I, Derici H, Paksoy S, Symptomatic duodenal lipoma with endoscopic snare polypectomyUlus Cerrahi Derg 2014 30(2):103-05. [Google Scholar]
[41]. Chang CW, Chu CH, Shih SC, Chen MJ, Yang TL, Chang WH, Duodenal polypoid lipoma with bleedingAm J Surg 2010 200(4):e49-50. [Google Scholar]
[42]. Weiss A, Mollura JL, Profy A, Cohen R, Two cases of complicated intestinal lipoma. Review of small intestinal lipomasAm J Gastroenterol 1979 72(1):83-88. [Google Scholar]
[43]. Whetstone MR, Zuckerman MJ, Saltzstein EC, Boman D, CT diagnosis of duodenal lipomaThe American Journal of Gastroenteroly 1985 80(4):251-52. [Google Scholar]
[44]. Abu Daff SN, Abu Daff NS, Laparoscopic enucleation of a duodenal lipoma, with review of the literatureSaudi Med J 2008 29(3):455-57. [Google Scholar]
[45]. Agha FP, Dent TL, Fiddian-Green RG, Braunstein AH, Nostrant TT, Bleeding lipomas of the upper gastrointestinal tract. A diagnostic challengeAm Surg 1985 51(5):279-85. [Google Scholar]
[46]. Munson FA, Duodenal lipoma. A report of two cases with a review of the literatureAm J Gastroenterol 1972 58(6):613-18. [Google Scholar]
[47]. Hizawa K, Kawasaki M, Kouzuki T, Aoyagi K, Fujishima M, Unroofing technique for the endoscopic resection of a large duodenal lipomaGastrointest Endosc 1999 49(3 Pt 1):391-92. [Google Scholar]
[48]. Sarma DP, Weilbaecher TG, Basavaraj A, Reina RR, Symptomatic lipoma of the duodenumJ Surg Oncol 1984 25(2):133-35. [Google Scholar]
[49]. Imamura K, Fuchigami T, lida M, Ohgushi H, Omae T, Kimura Y, Duodenal lipoma–a report of three casesThe American Society for Gastrointestinal Endoscopy 1983 29(3):223-24. [Google Scholar]
[50]. Barr WBJ, Yamashita T, Lipoma of the duodenum causing massive melenaAm J Gastroenterol 1964 41:418-22. [Google Scholar]
[51]. Yong P, Bing-Yin Z, Tao W, Li-Jun T, Fu-Zhou T, Unroofing and grasp-and-snare techniques in the management of a large, duodenal lipoma by duodenoscope combined with a double-channel endoscopeGastrointest Endosc 2014 79(1):27 [Google Scholar]
[52]. Lukash WM, Osborne DP, Brown LT, Russo JF, Lipoma of duodenum. Report of a caseAm J Gastroenterol 1968 49(6):494-98. [Google Scholar]
[53]. Thorlacius H, Weiber H, Ljungberg O, Nielsen J, Toth E, Endoscopic diagnosis and treatment of a giant duodenal lipoma presenting with gastrointestinal bleedingEndoscopy 2013 45(Suppl 2 UCTN):E385-86. [Google Scholar]
[54]. Ouwerkerk HM, Raber Freling G, Klaase JM, Duodenal lipoma as a rare cause of upper gastrointestinal bleedingGastroenterology Res 2010 3(6):290-92. [Google Scholar]
[55]. Smith FR, Mayo CW, Submucous lipomas of the small intestineAm J Surg 1950 80(7):922-28. [Google Scholar]
[56]. Carney JA, Stratakis CA, Stromal, fibrous, and fatty gastrointestinal tumours in a patient with a PDGFRA gene mutationAm J Surg Pathol 2008 32(9):1412-20. [Google Scholar]
[57]. Jeong IH, Maeng YH, Gastric lipomatosisJ Gastric Cancer 2010 10(4):254-58. [Google Scholar]
[58]. Chen HT, Xu GQ, Wang LJ, Chen YP, Li YM, Sonographic features of duodenal lipomas in eight clinicopathologically diagnosed patientsWorld J Gastroenterol 2011 17(23):2855-59. [Google Scholar]
[59]. Genchellac H, Demir MK, Ozdemir H, Computed tomographic and magnetic resonance imaging findings of asymptomatic intra-abdominal gastrointestinal system lipomasJ Comput Assist Tomogr 2008 32(6):841-47. [Google Scholar]
[60]. Yu HG, Ding YM, Tan S, Luo HS, Yu JP, A safe and efficient strategy for endoscopic resection of large, gastrointestinal lipomaSurg Endosc 2007 21:265-69. [Google Scholar]
[61]. Downs-canner S, Van der vliet WJ, Thoolen SJ, Robotic surgery for benign duodenal tumoursJ Gastrointest Surg 2015 19:306-12. [Google Scholar]