The traditional definition for ED is inability to achieve and/or maintain an erection for satisfactory sexual intercourse [1]. It can affect men of all ages, but prevalence increases with age and can affect up to 52 percent men between age group of 40-69 years [2].
Before 1980s, psychotherapists dominated the terrain of evaluation of ED, but with the introduction of Papaverine in 1982 by Virag R, testing by intracavernosal injection of pharmacological agents became a well accepted procedure in the evaluation of ED [3]. The sonographic evaluation of ED was pioneered by Lue TH et al., [4]. They hypothesised that 75% increase in the diameter of cavernosal artery subsequent to intracavernosal injection of vasodilating agents is good sign of normal arterial flow.
The ED is largely classified into two categories; ‘psychologic’ and ‘organic’. Vasculogenic causes are the most common aetiology of organic impotence. Vascular ED can be explained by two mechanisms i.e., obstruction in penile inflow tract which leads to arterial insufficiency or inability to trap the incoming blood in the cavernosa, also known as veno-occlusive dysfunction [5].
Pharmaco Penile Duplex Ultrasonography (PPDU) can be performed by oral or intracavernosal vasoactive agents. Intracavernosal injection of papaverine causes erection by direct smooth muscle relaxation and consequent filling of the corpus cavernosum with blood. However, intracavernosal injections are painful and associated with fear, anxiety, haematoma, risk of extravasation and priapism [6].
Tadalafil is a Phosphodiesterase type 5 (PDE5) inhibitor marketed in pill form for treating ED. Tadalafil’s pharmacologic distinction is its longer half-life (17.50 hours) compared to Sildenafil and Vardenafil (both 4.0-5.0 hours). Oral Tadalafil has been studied for non invasive evaluation of ED as an alternative to intracavernosal injection of vasoactive drugs. Unlike intracavernosal agents, Tadalafil alone cannot achieve satisfactory erection and it must be supplemented with audiovisual sexual stimulation and the results are inconsistent [7]. The quality of erection and the PSV achieved with oral pharmacological agents is lower than the same parameters achieved after intracavernosal injection [8].
At present institute, most of the patients who were being referred for evaluation of ED with PPDU were having normal doppler findings. So the study was done to evaluate the efficacy of oral PDE5 inhibitors and to avoid invasiveness of Papaverine, mainly in patients with psychogenic impotence and to assess whether it can replace intracavernosal Papaverine in the evaluation of ED. The present study aimed to assess whether oral Tadalafil is as useful as injectable Papaverine in the evaluation of men with ED.
Materials and Methods
A prospective longitudinal study was conducted in Department of Radiology, Nizam’s Institute of Medical Sciences, Hyderabad, India over a period of two years (6th August 2015 to 5th August 2017) in a selected population of 36 patients. All procedures were done in accordance with the standards of the Institutional Ethics Committee.
Inclusion Criteria
The present study population included male patients of all ages, both married and unmarried who were being evaluated for ED and were referred from Department of Urology.
Exclusion Criteria
Patients who were known cases of trauma, postoperative status for some other penile pathologies, Peyronie’s disease and intracavernosal injections/PDE5-inhibitors contraindications such as recent myocardial infarction, coagulation defects, severe ischaemia, poor cardiac performance and nitrates or nitric oxide donors taken in any form either regularly or intermittently were excluded from this study.
Technique
The individual information, clinical history and findings of every patient were recorded in a prescribed format. Informed consent was taken from all patients.
All cases were performed on E-Soate My Lab 60 Ultrasound-colour Doppler system with linear broadband phased array transducer (7-12 MHz).
Pharmaco penile duplex ultrasonography was done in all patients with two protocols with one week gap. First one was ‘Tadalafil mode’ and second one was ‘Papaverine mode’.
Tadalafil mode: Patients were given oral Tadalafil (20 mg), two hours before the procedure. An audiovisual self stimulation and self-genital stimulation were performed 10 minutes before the test.
Papaverine mode: After one week patients underwent penile doppler study following intracavernosal injection with Papaverine (60 mg).
In both protocols, gray scale imaging followed by duplex ultrasonography was done. Spectral waveforms were recorded once in five minutes for half an hour. Cavernosal artery diameter, PSV, EDV, AT and RI were recorded in all patients. The erectile response is categorised visually from E0 to E5 as proposed by Broderick GA and Arger P [9]. The average time spent by study group in the Ultrasonography room was 40-45 minutes during each study.
Statistical Analysis
The results were presented in number for the data in tables. All the data was analysed using SPSS software version 22.0 (SPSS Inc., Armonk, NY, USA). Pearson’s Chi-square, p-value and t-test were calculated. Statistical significance was accepted when p<0.05.
Results
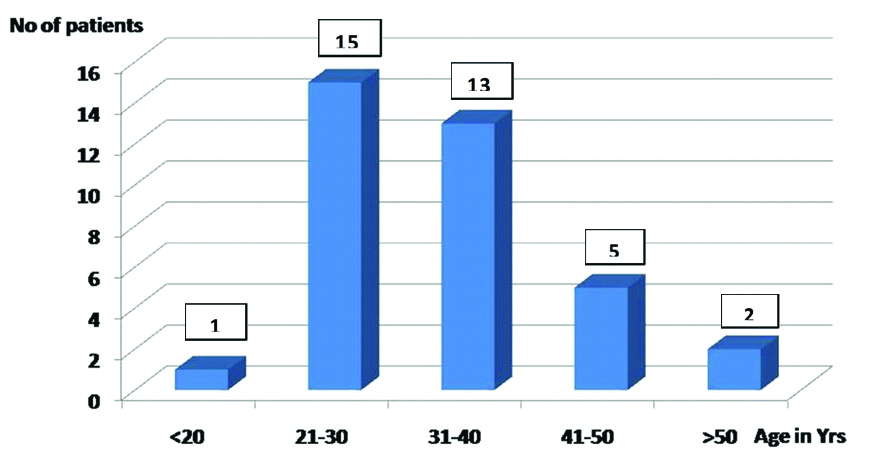
In the present study, we selected 36 patients between the age group of 18-65 years with mean age of 34.1 years. Patients between age group of 21-30 years constitute the dominant group (41.6%) [Table/Fig-1].
Age wise distribution of number of patients.
Diabetes mellitus was present in four patients, hypertension in five patients, coronary artery disease in one patient and peripheral vascular disease in one patient.
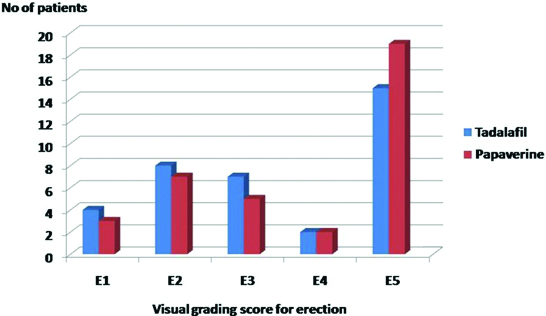
In Tadalafil mode, visual grading for erectile response was E1 in four patients, E2 in eight patients, E3 in seven patients, E4 in two patients and E5 in 15 patients. In Papaverine mode, visual grading for erectile response was E1 in three patients, E2 in seven patients, E3 in five patients, E4 in two patients and E5 in 19 patients [Table/Fig-2]. In the present study, for visual grading of erectile response in both modes, Pearson’s Chi-square was 5.535 and p-value was 0.237 that means there was no statistical significant difference in erection scores with Tadalafil or Papaverine.
number of patients with different visual garding scores for erectile response.
In the present study, cavernosal artery diameter before using any drug was 0.4-0.7 mm with mean of 0.49 mm. In Tadalafil mode, it varied from 0.6-1.4 mm with mean of 0.87 mm and in Papaverine mode, it varied from 0.5-1.8 mm with mean of 0.97 mm.
In total, mean PSV was 28.97 cm/second with Tadalafil and 36.72 cm/second with Papaverine. A t-test was 2.25 and p-value was 0.027, that means this finding was statistically significant.
All patients with visual grading response for erection E4 and E5 in Tadalafil mode showed mean PSV of 37.3 cm/second and in Papaverine mode showed mean PSV of 49.5 cm/second.
EDV was >5 cm/second and RI was <0.7 in two cases of venous insufficiency in both modes. In all other patients EDV and RI values were normal. AT values were normal in all patients (<100 m/second).
In Tadalafil mode, a total of 17 (47.2%) patients with grading score for erection E4 and E5 showed no evidence of arterial or venous insufficiency. A total of 17 (47.2%) patients showed evidence of arterial insufficiency (Visual grading response for erection is E1 in four patients, E2 in seven patients and E3 in six patients), 2 (5.5%) patients showed evidence of venous insufficiency (Visual grading response for erection is E2 in one patient and E3 in one patient).
In Papaverine mode, a total of 21 (58.3%) patients with grading score for erection E4 and E5 showed no evidence of arterial or venous insufficiency. A total of 12 (38.3%) patients showed evidence of arterial insufficiency (Visual grading response for erection is E1 in three patients, E2 in six patients and E3 in three patients), 2 (5.5%) patients showed evidence of venous insufficiency (Visual grading response for erection is E2 in one patient and E3 in one patient) and 1 (2.7%) patient showed indeterminate results (Visual grading response for erection is E3) [Table/Fig-3].
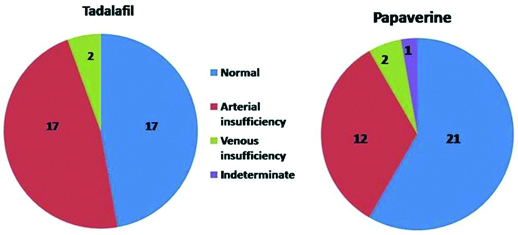
Final PPDU impression with number of patients in each category.
Discussion
The mechanism of ED is a multi phase event involving vascular, endocrinologic, pharmacologic, neurologic or psychogenic problems [10].
The PPDU provides reliable and detailed information on penile vascular anatomy and haemodynamics and is recommended as a first-line test to evaluate penile arterial and veno-occlusive function [9]. It can be performed by oral or intracavernosal vasoactive agents.
Intracavernosal injections can cause pain, ecchymosis, haematoma and priapism. Also, fear of injection can lead to stress, anxiety and increased sympathetic stimulation that may result in a false-positive response. Shamloul R, revealed that PSV may be falsely lowered in young patients after the first intracavernosal injection which might need repetition of the study [11]. However, it was rarely accepted by the patients in clinics. So in the present study, we tried to investigate the potential use of oral Tadalafil administration which is PDE5 Inhibitor and to assess whether it can replace intracavernosal Papaverine in the evaluation of ED.
Tadalafil differs from Papaverine, both in molecular structure and mechanism of action. Papaverine increases the production of cyclic guanosine monophosphate and cyclic adenosine monophosphate by an inhibitory action on PDE, leading to a very complex mode of action in the smooth muscle. On the other hand, Tadalafil maintains an erection by inhibiting the catabolism of cyclic guanosine monophosphate, resulting in increase of the same. So, the activation of the nitric oxide-cyclic guanosine monophosphate pathway by sexual stimulation is required. Thus, in the absence of sexual stimulation, Tadalafil has little effect on cavernosal smooth muscle relaxation and does not cause rigid penile erection [12].
In normal individuals, cavernosal artery diameter ranges from 0.2-1 mm [1]. In flaccid state, on colour doppler the arterial flow is difficult to visualise. However, sometimes damped and monophasic systolic wave form with minimal diastolic component can be seen. Erectile response, increase in cavernosal artery diameter and vascular flow were analysed in post drug status. The erectile response was graded visually from E0 to E5 in all patients as suggested by Broderick GA Arger P [Table/Fig-4] [9].
Broderick GA and Arger P visual garding score for penile erection during PPDU.
| EO | No Response |
|---|
| E1 | Elongation of shaft only |
| E2 | Moderate tumescence, no rigidity |
| E3 | Full tumesence, no rigidity, easly bendable |
| E4 | Full erection, partial rigidity |
| E5 | Full rigidity for atleast 20 minutes |
Five phases have been described in normal spectral waveform [13]. In phase 1, increase in both systolic and diastolic velocities. Phase 2 shows progressive decrease in end diastolic velocity and appearance of dicrotic notch. In phase 3, diastolic flow approaches to zero and it is reversed in phase 4. Phase 5, shows eventual loss of both systolic and diastolic signals.
Normal flowmetry reference values during PPDU are: PSV-25 cm/second or more, EDV-5 cm/second or less, AT-0.11 seconds or less and RI-0.85 or more [1]. Arterial insufficiency is suggested by less than 75% increase in baseline cavernosal artery diameter, abnormal PSV (less than 25 cm/second) and AT (more than 0.11 seconds) [Table/Fig-5]. Veno-occlusive disease is suggested by abnormal RI (less than 0.85) and EDV (more than 5 cm/ second) [Table/Fig-6] [10].
A case of arterial insufficiency.
Veno-occlusive disease-EDV is more than 5 cm/second.
Increase in mean Cavernosal Artery Diameter (CAD) was more with Papaverine than with Tadalafil. However, t-test was 1.543 and p-value was 0.127 that means, this finding was statistically not significant.
From the aspect of PSV, one study done by Yang Y et al., showed that statistically, there was no difference for PSV between Tadalafil and Papaverine [7]. But in the present study, mean PSV was more with Papaverine. A t-test was 2.25 and p-value was 0.027 that means there was statistically significant difference between these two.
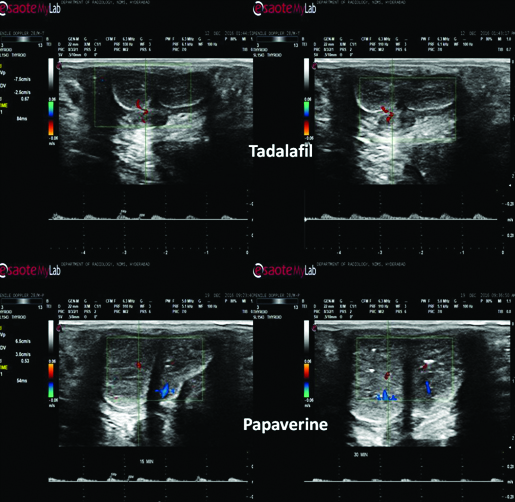
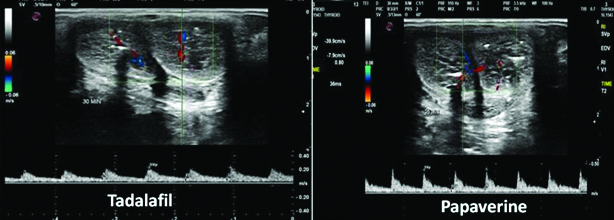
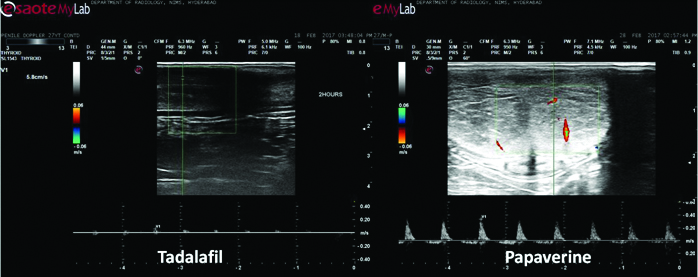
Five cases of arterial insufficiency by Tadalafil mode proved to be normal by Papaverine mode. In all these patients maximum PSVs achieved with Papaverine were in borderline range (30-35 cm/second). Papaverine proved to be more effective in these patients [Table/Fig-7].
Tadafil mode shows arterial insufficiency, however Papaverine mode showed normal study.
From the aspect of EDV, RI and AT, Pearson’s Chi-square was zero and p-value was 1, that means no statistically significant difference between Tadalafil and Papaverine.
In Tadalafil mode, a total of 17 patients showed no evidence of arterial or venous insufficiency, 17 patients showed evidence of arterial insufficiency and two patients showed evidence of venous insufficiency. In Papaverine mode, a total of 21 patients showed no evidence of arterial or venous insufficiency, 12 patients showed evidence of arterial insufficiency, two patients showed evidence of venous insufficiency and one patient showed indeterminate results. Pearson’s Chi-square was 2.283 and p-value was 0.516 that means statistically no significant difference between Tadalafil and Papaverine. These findings (EDV, RI, AT and final diagnosis) were similar to the study done by Yang Y et al., [7].
In the present study, one patient had developed priapism (0.3%) following intracavernosal injection of Papaverine, which was of low flow in nature and treated by emergency decompression by urologist. These findings are similar to a study by Kilic M et al., [14].
In the present study, oral Tadalafil had significantly contributed in the evaluation of ED. Even though intracavernosal Papaverine is proved to be the gold standard, this technique has the advantages of being fast, easily available, cost effective and the results are highly accurate [13]. The disadvantages are low PSV values and slightly lower quality of erection with Tadalafil in both normal and arterial insufficiency patients.
Limitation
The limitations in the present study are relatively small sample size and requirement of self sexual stimulation in an unfamiliar environment in Tadalafil mode and chances of priapism with Papaverine mode.
Conclusion
In conclusion, Tadalafil and Papaverine showed statistically significant results similar to each other. Tadalafil is more useful in psychogenic impotence as this avoids invasiveness of Papaverine. However, more patients had better response to Papaverine in the form of better erection response and high PSVs, whereas Tadalafil administration still showed some pitfalls in practical use.