Validity and Reproducibility of Digital Models Obtained by Cone Beam Computed Tomography Imaging
Apurva Bariar1, Fidha Nazeer2, Nidhin Philip3, Siddarth Shetty4
1 Consulting Orthodontist, Tooth Cave, Jangpura Extension, New Delhi, India.
2 Postgraduate Student, Department of Orthodontics, Manipal College of Dental Sciences, Mangaluru, Karnataka, India.
3 Reader, Department of Orthodontics, Manipal College of Dental Sciences, Mangaluru, Karnataka, India.
4 Professor and Head, Department of Orthodontics, Manipal College of Dental Sciences, Mangaluru, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Fidha Nazeer, Postgraduate Student, Department of Orthodontics and Dentofacial, Orthopaedics, Manipal College of Dental Sciences, Light House Hill Road, Mangaluru-575001, Karnataka, India.
E-mail: fidha.nazeer@gmail.com
Introduction
Impression making and fabrication of plaster models serve as a basis for documentation, diagnosis and treatment planning. Model analysis is used routinely in orthodontics and is a key factor for treatment planning and review of orthodontic progress. Recently newer technologies in imaging and digitalisation have made it possible to obtain 3-Dimensional (3D) virtual models. Virtual models score over plaster models with respect to accessibility, storage and long life. However, there are concerns over its accuracy and reproducibility.
Aim
To evaluate the accuracy of three dimensional digital models obtained from Cone Beam Computed Tomography (CBCT).
Materials and Methods
This was an ex-vivo study. Thirty dental models of patients were selected and scanning of these models were done using CBCT. Means and standard deviations of the space analysis measurements were calculated by using both plaster and digital models. Statistical analyses were used to investigate the accuracy and repeatability of the methods studied using Statistical Package of Social Sciences (SPSS) 20.0. Paired t-tests for both mean and standard errors were calculated.
Results
The results for all 30 maxillary and mandibular models were similar. There was a statistically significant difference in calculating sum of ten teeth for both maxillary and mandibular teeth between the plaster and dental digital models and in mesio distal measurements between digital and plaster dental models.
Conclusion
Digital models provide a more accurate measurement of mesio distal width of tooth with a statistically significant difference of (p-value=0.002).
CBCT, Digital models, Mesio-Distal Widths
Introduction
Obtaining accurate records is essential for effective orthodontic diagnosis and treatment planning. Historically this need was satisfied by 2-Dimensional (2D) and 3D representations, of which study models were the only 3D component [1]. Models provide information for diagnosis and treatment planning and function as a 3D record of the pretreatment malocclusion [2]. Through advances in biomaterials, it is now possible to obtain robust and dimensionally accurate dental plaster models and these have long been the gold standard in orthodontics [3].
Transition to electronic dental records have been seen in many clinical practices which includes everything from medical histories and progress notes to radiographs and models which are now available in a digital format [4,5]. When considering the huge storage space required for traditional plaster casts, this format is particularly advantageous as digital models eliminate the need for large storage rooms, susceptibility to damage and their associated expenses [4-9].
Incremental information obtained from different types of diagnostic records contributes to the determination of orthodontic treatment decisions [10]. The integration of digital 3D models with existing 3D imaging technologies such as Cone-Beam Computed Tomography (CBCT) and 3D photography has already been described in literature [11,12]. There will soon be a true 3D reconstruction of the patient’s craniofacial complex for orthodontic diagnosis, treatment planning, progress, and outcome assessment. Also, digital 3D models printing are possible with a rapid prototyping technology if a physical model of the dentition is needed: e.g., for the manufacture of orthodontic appliances [4]. However, it carries a disadvantage of temporarily or forever losing the models if a computer failure were to occur [13,14].
There are various methods of digitization that has been seen in literature which include intraoral scanning, 3D laser scanning systems with cameras [1] etc. Here digitizing of the models were done using CBCT. The aim of the current study was to evaluate the accuracy of measurements obtained from 3 Dimensional digital models obtained from CBCT.
Materials and Methods
This was an ex-vivo study which was done in a period of one month from 1st Januray 2016 to 31st Januray 2016 after attaining approval from the Institutional Ethics Committee, Manipal College of Dental Sciences, Manipal Academy of Higher Education, Mangaluru, Karnataka, India. Informed Consent from all the patients was taken prior to the commencement of the study. Patient records from the Department of Orthodontics and Dentofacial Orthopedics of Manipal College of Dental sciences, Mangaluru, were selected.
The Inclusion criteria included: 1) Permanent dentition from left first molar to right first molar in both arches; 2) Normal dental crown morphology; 3) Patients who hadn’t undergone fixed Orthodontic treatment; 4) Patients without severe crowding (More than 6 mm). Patients who had features that would influence crown morphology such as restorations, caries, attrition, or fracture were excluded from the study.
Thirty dental models of patients who met these criteria were randomly selected for the study (Poured with dental stone-DENSTONE).
CBCT scanning of all the 30 models were done using - PlanmecaPromax 3D Mid Model with Romexis Software version 3.2.1, Heksinki, Finland with Model scanning program using orthostudio software at the Department of Oral Medicine and Radiology, MCODS, Mangalore. For each patient, impressions were taken with alginate impression material (Zelgan plus -DENTSPLY) and two types of dental models were analysed - CBCT obtained digital dental models and plaster dental models.
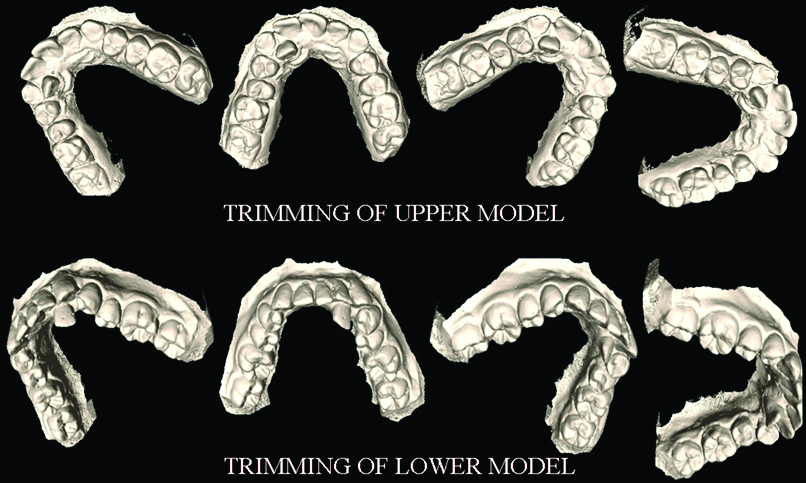
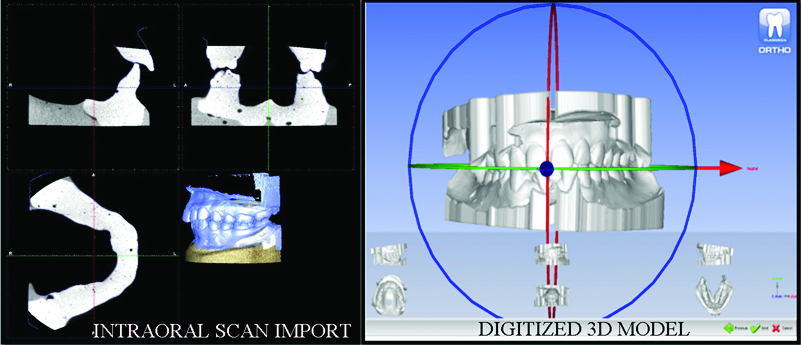
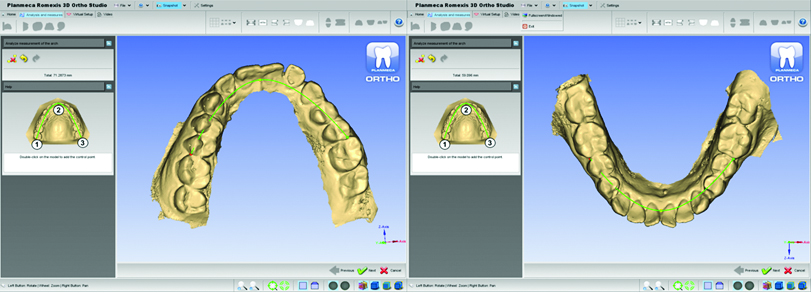
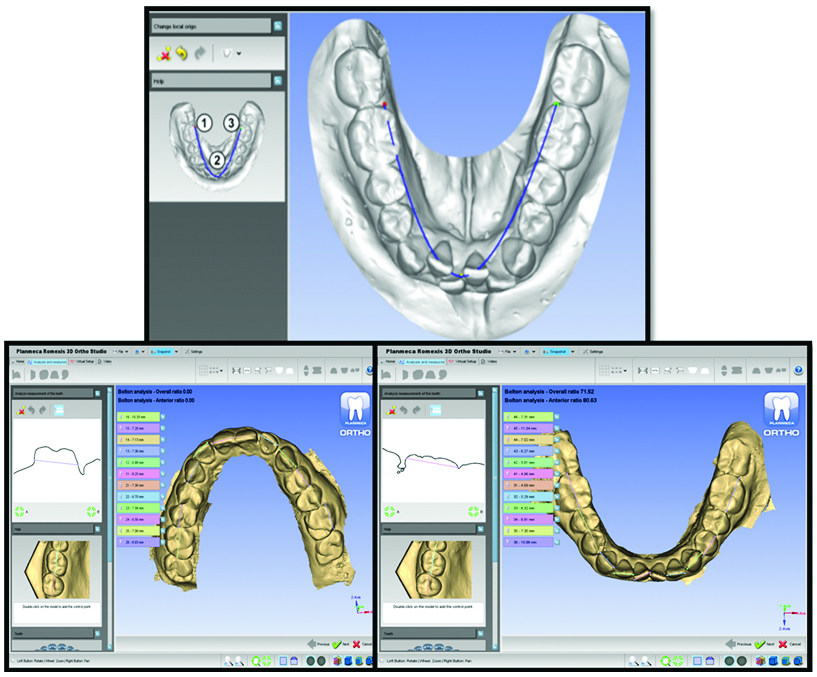
To process the digital models, three CBCT scans were taken of each plaster dental model-Exposure of maxillary and mandibular plaster dental model by selecting model capture from Planmeca Romexis and the bite index by selecting 3D capture from the program. The image of the bite index was in DICOM format and maxillary and mandibular model was in STL format. Upper model was opened from PlanmecaRomexis volumes list and trimming of the model was done which was repeated for the lower model [Table/Fig-1]. Upper and lower models were imported in STL format by marking the corresponding points on the bite index. Models were then launched in PlanmecaRomexis 3D Ortho studio to get digitized models [Table/Fig-2]. Correct orientations of the models were made. Mesio distal measurements of all teeth were made on the digital models from the analysis and measurement icon [Table/Fig-3]. Arch length measurement was made by clicking the measure arch icon [Table/Fig-4]. Similar measurements were made on the plaster dental models using digital caliper to measure the greatest mesiodistal widths to 1 mm [Table/Fig-5]. Sum of maxillary and mandibular ten teeth were calculated and compared in both the situations. The arch length of the dental plaster model was constructed by bending a piece of brass wire over the contact points of the posterior teeth, tips of canines and incisal edges of centrals and laterals from 1st molar to 1st molar. Arch perimeter analysis was done manually for the plaster model and with 3D ortho studio software on digital dental models.
A 3D Trimming of Upper and Lower models.
Intraoral scan import and Digitized 3D Model.
Arch perimeter and carey’s analysis measured in Orthostudio.
Mesio-Distal dimensions of tooth.
Manual measurement of the mesio-distal dimensions of tooth.

Statistical Analysis
Statistical analyses were used to investigate the accuracy and repeatability of the methods studied using SPSS 20.0. Means and standard deviations of the space analysis measurements were calculated by using both plaster and digital models to obtain data. These were compared using paired t-test to determine the validity of the digital measurements. Intraobserver error was eliminated by taking an average of two measurements.
Results
The mean value for sum of ten teeth for maxillary plaster models was 73.4(SD 5.03) and for digital models were 72.5(SD 4.79). For mandibular models, mean values for plaster models were 65.05 (SD 3.765) and for digital models were 64.03 (SD 3.626). Statistically significant difference exists between the two (p-value=0.002) [Table/Fig-6].
Paired t-test to compare the differences between the actual and the digital measurements.
| Pairs | Parameters | Mean | Std. Deviation | p-value |
|---|
| Pair 1 | Mx arch pm | 70.25 | 4.5367 | 0.173* |
| Mx arch pm digital | 69.9 | 4.2939 |
| Pair 2 | Mnd arch pm | 61.217 | 3.8117 | 0.177* |
| Mnd arch pm digital | 60.783 | 3.6992 |
| Pair 3 | S 10 mx | 73.417 | 5.0311 | 0.002* |
| S 10 mx digital | 72.517 | 4.7967 |
| Pair 4 | S 10 mnd | 65.05 | 3.7654 | 0.002* |
| S 10 mnd digital | 64.033 | 3.6268 |
| Pair 5 | Upper diff | 4.983 | 3.5489 | 0.064 |
| Upper diff digital | 4.657 | 3.4579 |
| Pair 6 | Lower diff | 3.9 | 2.6794 | 0.533 |
| Lower diff digital | 4.067 | 2.5418 |
* statistically significant at p<0.05
The mean value for arch perimeter for maxillary plaster models was 70.25 (SD 4.53) and for digital models was 69.9 (SD 4.29). For mandibular models, mean values for plaster models were 61.21 (SD 3.81) and for digital models were 60.78 (SD 3.69). The p-value from the paired t-test for maxillary and mandibular models obtained was 0.173 and 0.177 which showed no statistically significant difference exist between the two.
The mean value for difference between sum of 10 and arch perimeter length (arch perimeter analysis) for maxillary plaster models was 4.98 (SD 3.54) and for digital models was 4.65 (SD 3.45). For mandibular models, mean values for plaster models were 3.9 (SD2.67) and for digital models were 4.06 (SD 2.54). A p-value from the paired t-test for maxillary and mandibular models obtained was 0.064 and 0.533 which showed no statistically significant difference exist between the two.
Discussion
The trend to perform virtual model analysis has been increasing exponentially and different software programmes are available for the same purpose.
In the present study, the results for both maxillary and mandibular models were similar. There was a statistically significant difference in, calculating sum of ten, between the plaster and dental digital models.
According to the present study, statistically significant difference exists in mesio distal measurements between digital and plaster dental models. But while comparing the arch perimeter of the two, no statistically significant difference was found. There are various advantages of performing model analysis on digital models using ortho studio such as clear visibility of tooth edges in various planes, better acknowledgement of greatest mesiodistal width of the tooth and a definite curve while measuring arch perimeter showing a more definite and accurate measurement as compared to manual measurements of plaster dental models [Table/Fig-4]. Preliminary results indicated that digital models are not a compromised choice for treatment planning or diagnosis as shown in a study done by Stevens DR et al., in 2006 which compared the validity, reliability and reproducibility of plaster vs digital models [7], analysed tooth sizes and occlusal relationships - specifically the Bolton’s analysis and Peer Assessment Rating (PAR) index and their component.
Systematic review by Fleming PS and Marinho VJA, and by Rossini G et al., concluded that Digital models offer a high degree of validity, reliability and reproducibility when compared to direct measurement on plaster models; differences between the approaches are likely to be clinically acceptable [15,16]. The above-mentioned studies support the accuracy of digital dental models.
In a study done by Wiranto MG et al., validity, reliability and reproducibility of linear measurements on digital models obtained from intraoral and Cone Beam Computed Tomography scans of alginate impressions was compared [17]. They concluded that both are valid, reliable and reproducible methods of obtaining dental measurements for diagnostic purposes.
Limitation
In the present study, care was taken to orient all the dental models in the same plane while taking the scans. But at the same time, there maybe a few drawbacks in this study - It can be time consuming to locate the greatest height of contour and reproducibility of defects in plaster dental models. In order to overcome this, direct intra oral scanner can be used and studies on determining their accuracies can be done.
Conclusion
Digital models provide a more accurate measurement of mesio distal width of tooth. Arch perimeter analysis did not show any significant difference between the digital and plaster dental models. Although, direct intraoral scanning would provide a better accuracy in terms of records as the error that has been incorporated in plaster models are reproduced in the digital models while scanning them, intraoral scans are more expensive and are not widely in use in today’s era. Further studies can be done to evaluate the accuracy of digital models obtained from direct intra oral scans.
* statistically significant at p<0.05
[1]. White AJ, Fallis DW, Vandewalle KS, Analysis of intra-arch and interarch measurements from digital models with 2 impression materials and a modeling process based on cone-beam computed tomographyAm J Orthod Dentofac Orthop [Internet]. American Association of Orthodontists 2010 137(4):456.e1-456.e9.10.1016/j.ajodo.2009.09.01920362900 [Google Scholar] [CrossRef] [PubMed]
[2]. Sweeney S, Smith DK, Messersmith M, Comparison of 5 types of interocclusal recording materials on the accuracy of articulation of digital modelsAm J Orthod Dentofacial Orthop 2015 148(2):245-52.10.1016/j.ajodo.2015.04.02526232833 [Google Scholar] [CrossRef] [PubMed]
[3]. Akyalcin S, Cozad BE, English JD, Colville CD, Laman S, Diagnostic accuracy of impression-free digital modelsAm J Orthod Dentofac Orthop [Internet]. American Association of Orthodontists 2013 144(6):916-22.10.1016/j.ajodo.2013.04.02424286915 [Google Scholar] [CrossRef] [PubMed]
[4]. Quimby ML, Vig KW, Rashid RG, Firestone AR, The accuracy and reliability of measurements made on computer-based digital modelsAngle Orthod 2004 74(3):298-303. [Google Scholar]
[5]. Rheude B, Sadowsky PL, Ferriera A, Jacobson A, An evaluation of the use of digital study models in orthodontic diagnosis and treatment planningAngle Orthod [Internet] 2005 75(3):300-04. [Google Scholar]
[6]. Bell A, Ayoub AF SP, Assessment of the accuracy of a three-dimensional imaging system for archiving dental study modelsJ Orthod 2003 30(3):219-23.10.1093/ortho/30.3.21914530419 [Google Scholar] [CrossRef] [PubMed]
[7]. Joffle L, Ortho CAD: digital models for a digital eraJ Orthod 2004 31(4):344-47.10.1179/14653120422502667915608352 [Google Scholar] [CrossRef] [PubMed]
[8]. Mayers M, Firestone AR, Rashid R, Vig KW, Comparison of Peer Assessment Rating (PAR) index scores of plaster and computer-based digital modelsAm J Orthod Dentofac Orthop 2005 128(4):431-34.10.1016/j.ajodo.2004.04.03516214623 [Google Scholar] [CrossRef] [PubMed]
[9]. Creed B, Kau CH, English JD, Xia JJ, Lee RP, A Comparison of the accuracy of linear measurements obtained from cone beam computerized tomography images and digital modelsSemin Orthod [Internet] 2011 17(1)Elsevier Inc:49-56.10.1053/j.sodo.2010.08.01026568670 [Google Scholar] [CrossRef] [PubMed]
[10]. Han UK, Vig KW, Weintraub JA, Vig PS KC, Consistency of orthodontic treatment decisions relative to diagnostic recordsAm J Orthod Dentofac Orthop 1991 100(3):212-19.10.1016/0889-5406(91)70058-5 [Google Scholar] [CrossRef]
[11]. El-Zanaty HM, El-Beialy AR, Abou El-Ezz AM, Attia KH E-BA, YA. M, Three-dimensional dental measurements: an alternative to plaster modelsAm J Orthod Dentofac Orthop 2010 137(2):259-65.10.1016/j.ajodo.2008.04.03020152684 [Google Scholar] [CrossRef] [PubMed]
[12]. Baumgaertel S, Palomo JM, Palomo LHM, Reliability and accuracy of cone-beam computed tomography dental measurementsAm J Orthod Dentofac Orthop 2009 136(1):19-25.10.1016/j.ajodo.2007.09.01619577143 [Google Scholar] [CrossRef] [PubMed]
[13]. Lippold C, Kirschneck C, Schreiber K, Abukiress S, Tahvildari A, Moiseenko T, Methodological accuracy of digital and manual model analysis in orthodontics - A retrospective clinical studyComput Biol Med [Internet]. Elsevier 2015 62:103-09.10.1016/j.compbiomed.2015.04.01225917690 [Google Scholar] [CrossRef] [PubMed]
[14]. de Waard O, Rangel FA, Fudalej PS, Bronkhorst EM, Kuijpers-Jagtman AM, Breuning KH, Reproducibility and accuracy of linear measurements on dental models derived from cone-beam computed tomography compared with digital dental castsAm J Orthod Dentofac Orthop [Internet]. American Association of Orthodontists 2014 146(3):328-36.10.1016/j.ajodo.2014.05.02625172255 [Google Scholar] [CrossRef] [PubMed]
[15]. Fleming PS, Marinho VJA, Orthodontic measurements on digital study models compared with plaster models: a systematic reviewOrthod Craniofac Res 2011 14(1):01-16.10.1111/j.1601-6343.2010.01503.x21205164 [Google Scholar] [CrossRef] [PubMed]
[16]. Rossini G, Parrini S, Castroflorio T, Deregibus A, Debernardi CL, Diagnostic accuracy and measurement sensitivity of digital models for orthodontic purposes: A systematic reviewAm J Orthod Dentofacial Orthop 2016 149(2):161-70.10.1016/j.ajodo.2015.06.02926827972 [Google Scholar] [CrossRef] [PubMed]
[17]. Wiranto MG, Engelbrecht WP, Nolthenius HET, van der Meer WJ, Ren Y, Validity, reliability, and reproducibility of linear measurements on digital models obtained from intraoral and cone-beam computed tomography scans of alginate impressionsAm J Orthod Dentofacial Orthop 2013 143(1)10.1016/j.ajodo.2012.06.01823273370 [Google Scholar] [CrossRef] [PubMed]