Type-I Fused Deciduous Dentition in Mandibular Arch-Report of a Case and Clinical Considerations
Hemant Sawhney1, Anju Anu Jose2
1 Reader, Department of Oral Medicine and Radiology, School of Dental Sciences, Sharda University, Greater Noida, Uttar Pradesh, India.
2 Reader, Department of Oral Medicine and Radiology, School of Dental Sciences, Sharda University, Greater Noida, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Hemant Sawhney, Reader, Department of Oral Medicine and Radiology, School of Dental Sciences, Sharda University, Greater Noida, Uttar Pradesh-201310, India.
E-mail: omrd.sharda@gmail.com
Developmental anomalies of teeth are of clinical interest because of the problems associated with them. This report describes a unique case of unilateral fusion of primary mandibular lateral incisor and canine and discusses the possible future treatment options anticipated for management of fused deciduous teeth. Clinically, this case provides an insight into management options for fused deciduous teeth for general dental practitioners.
Bifid crown, Developmental anomaly, Double tooth, Fusion, Primary teeth
Fusion is described as the union of two distinct dental tooth buds, which may occur at any stage of the odontogenesis. It is a primary developmental anomaly and is also known by the terms ‘double tooth’, ‘twinning’, ‘double formation’, ‘joined teeth’ or ‘fused teeth’ [1]. Depending upon the stage of tooth development, fusion may be complete or incomplete causing pulp chambers and root canals to be joined/fused or separated [2]. The pathophysiology behind fusion is considered to be some physical force, perhaps pressure forcing young tooth germs into contact, causing necrosis of the intervening tissue and giving the enamel organ and the dental papilla an opportunity to unite [3]. A number of other reasons for this anomaly have been proposed, including trauma, environmental factors, evolution and heredity [4,5]. Moreover, fused teeth may form part of syndromes such as achondrodysplasia, chondroectodermal dysplasia, focal dermal hypoplasia, and osteopetrosis. Rarely dental fusion in natal teeth has also been reported in Ellis and Hallerman-streiff syndrome [6].
The prevalence of ‘twinning’ abnormalities is less than 1% [7]. Besides this, fusion is predominantly seen in the incisor and canine regions, more frequently in the mandibular incisor region than in the maxilla, and furthermore, more often in the primary than in the permanent dentition [8,9]. The prevalence of unilateral double tooth is 0.5% and that of bilateral double tooth is 0.02% [2]. Presented here is a case of unilateral type I fusion of primary right mandibular lateral incisor and canine, a morphological variant seen chiefly in maxilla [10].
A five-year-old boy presented for routine dental examination. The patient’s medical history was uneventful. Intra-oral clinical examination revealed that the patient had a full complement of deciduous dentition, a few decayed teeth and there was presence of a fused cuspid and lateral incisor in right mandibular arch with a groove between the two, up-to the middle third of the crowns [Table/Fig-1]. An initial carious lesion was noted on both labial and lingual grooves with plaque accumulation [Table/Fig-2].
Anterior view showing fused primary right mandibular lateral incisor and canine.

Palatal view showing initial carious lesion.

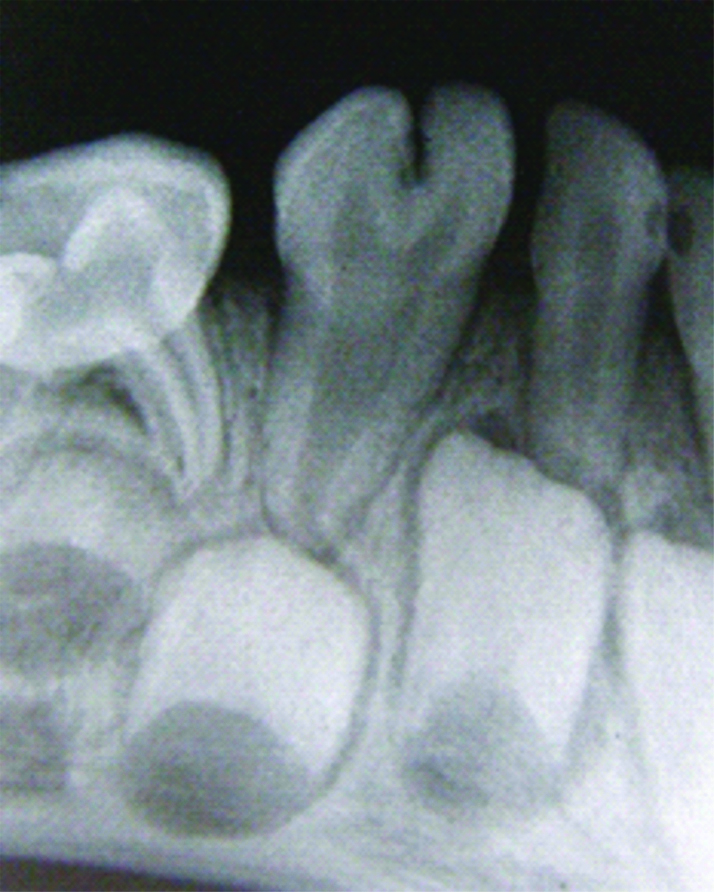
Periapical radiograph [Table/Fig-3] of the fused tooth revealed bifid crown (notching in the incisal third) with single root structure, a common pulp canal with separate pulp chambers. The succedaneous permanent lateral incisor was missing on the radiograph.
Periapical radiograph showing fused primary lateral incisor and canine with notching in the incisal 1/3rd with congenitally missing permanent lateral incisor.
A treatment plan for the child was made, which included restoration of carious teeth with latest generation of resin-modified light-cured glass ionomer cement because of its improved aesthetics and high fluoride release. The parent was counseled on the need for regular six months follow-up for radiographic evaluation of root resorption and space management.
Morphologically four different variants of fused teeth have been identified along with their specific distribution pattern in the arches [Table/Fig-4]. Our case presented with a Type 1 classification [10] which is Bifid Crown-Single Root. This type has larger than normal crown with a notch on the incisal edge, a bifid pulp chamber, normal sized root and radicular canal with a widening in the cervical portion. Hatice A et al., examined 40 patients with Primary Fused Teeth (PFT) and found that Type 1 is confined only to the maxillary teeth and mandibular lateral incisors and canines were the most common PFT. The most prevalent type of PFT in their study was Type III followed by Type I, IV and II. Carious involvement was more common with Type III and IV. They concluded that fusion related tooth aplasia and talon cusp were the anomalies which would be associated with Type I [9].
Agulio’s classification for different morphological types of fused teeth and their distribution patterns in the arches [10]. ‘+’ indicates usually present, ‘-’ usually absent.
| Morphological Variant | Description | Maxilla | Mandible |
|---|
| Type-1 (Bifid Crown-Single Root) | A larger than normal crown with a notch on the incisal edge. A bifid pulp chamber, normal sized root and radicular canal with a widening in the cervical portion. | + | - |
| Type-2 (Large Crown-Large Root) | A larger than normal crown, usually with no groove or notch. A single, shared large pulp chamber. A root that is wider than normal along all its length. One large shared root canal. | - | + |
| Type-3 (Two fused crowns-Double conical roots) | Two crowns, more or less well defined, with a vertical groove that goes in a cervical direction. The cervical portion of both crowns may be joined if the groove is partial. The groove can also be total, dividing the whole of the fused crowns, which may be symmetrical, or show distinct differences in form. The pulp chambers may be separate. A larger than normal root with a conical shape. It is not possible to make some separation between the two roots involved. The pulp canal may be shared in the coronal portion of the root, and end in two radicular canals. | - | + |
| Type-4 (Two fused roots) | Two crowns similar to Type-3. Two (or more) clearly distinct but joined roots, with two separate root canals. | + | + |
Only 15 cases of bilateral fusion of mandibular primary lateral incisors and canines have been reported in literature since 1940. Hagman FT reported that such patients have a 75% chance of lacking the succedaneous lateral incisor [11,12]. Rajashekhara BS et al., however, reported a case of bilateral fusion of primary mandibular lateral incisors and canines without any aplasia of permanent successors [13].
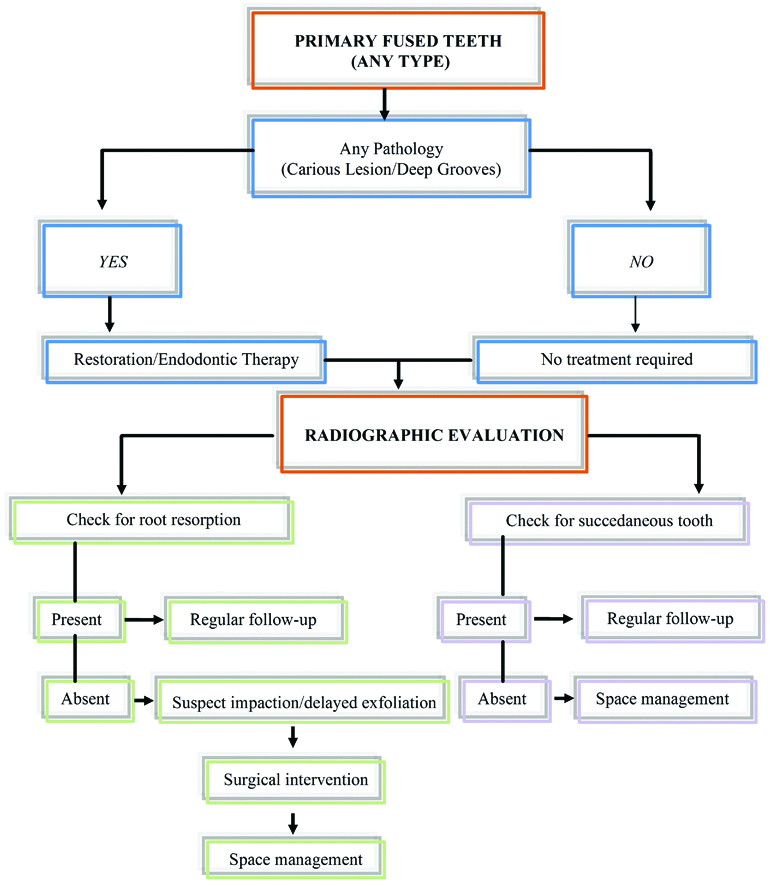
For treatment planning [Table/Fig-5] besides aesthetic problems, joined teeth are of interest for other clinical problems such as caries, abscesses, and fistulae, which may require some kind of endodontics, prosthetic and surgical treatment. Moreover, delayed exfoliation and anomalies in the permanent dentition such as impaction of the successors, diastemas, periodontal problems, supernumerary teeth, or aplasia of the teeth have been described [14].
Algorithm showing management options for fused primary teeth.
Fused teeth usually show an increased risk for dental caries as a result of conditions favoring dental plaque accumulation along the grooves between the crowns. Treatment plan for such type of anomalies should include a preventive resin restoration, like resin–based light–cured sealant in the grooves [15]. Most often, the permanent successor is found congenitally missing in the corresponding region [16]. In our patient, tooth bud of permanent lateral incisor was not evident on the radiograph. Although no treatment is recommended in the primary dentition, but regular radiographic evaluation is recommended to verify any effects on the succedaneous teeth or for early detection of presence or absence of permanent successors, which can allow dentist to plan treatment appropriately [17]. Although, conventional intraoral periapical radiographs provides sufficient information, advanced imaging modalities like micro CT and cone-beam CT should be used if endodontic/orthodontic intervention is planned as it facilitates more detailed view of complex and varied root canal system morphology. Data with low frequency of occurrence are often prized by forensic specialists and a single feature may hold sufficient weight to allow confirmation of identity [18]. A fused tooth with extremely low incidence could be used as an identification trait.
Conclusion
Usually fused teeth show an increased risk for dental caries due to dental plaque accumulation along the grooves between the crowns. Hence, clinical observation, along with radiographs, and intervention at the appropriate time are of utmost importance. These conditions require a minimal intervention approach, preventive procedures, and long-term follow-up.
[1]. Brook AH, Winter GB, Double Tooth: A retrospective study of ‘geminated’ and ‘fused’ teeth in childrenBritish Dental Journal 1970 129(3):123-30.10.1038/sj.bdj.48025335272471 [Google Scholar] [CrossRef] [PubMed]
[2]. Boyne PJ, Gemination: Report of two casesJ Am Dent Assoc 1955 50(2):194 [Google Scholar]
[3]. Monika R, Etiology of various dental developmental anomalies-review of literatureJournal of Dental Problems & Solutions 2017 4(2):19-25. [Google Scholar]
[4]. NikHussaein NN, Salcedo AH, Double teeth with hypodontia in identical twinsASDC J Dent Child 1987 54(3):179-81. [Google Scholar]
[5]. Shafer Hine Levy Textbook of Oral Pathology, 5th Edition; Developmental disturbances of Oral and Para-oral Structures:54-55. [Google Scholar]
[6]. Meena D, Mishra A, Singh C, Natal teeth with subesequent bilateral fusion of primary mandibular incisors-A Case ReportJournal of Advance Medical & Dental Sciences 2013 1(2):125-27. [Google Scholar]
[7]. Riesenberger RE, Killian CM, Triplication and twinning in one dental arch: Report of a caseQuintessence Int 1990 21(8):621-23. [Google Scholar]
[8]. Peretz B, Brezniak N, Fusion of primary mandibular teeth: Report of a caseASDC J Dent Child 1992 59(5):366-68. [Google Scholar]
[9]. Hatice A, Sevgin I, Emine ST, Primary fused teeth and finding in permanent dentitionMed Princ Pract 2018 27:129-32.10.1159/00048732229402820 [Google Scholar] [CrossRef] [PubMed]
[10]. Agulio L, Gandia J.L, Cibrian R, Catala M, Primary double teeth: A retrospective clinical study of their morphological characteristics and associated anomaliesInternational Journal of Pediatric Dentistry 1999 9(3):175-83.10.1046/j.1365-263x.1999.00131.x10815574 [Google Scholar] [CrossRef] [PubMed]
[11]. Chalakkal P, Thomas AM, Bilateral fusion of mandibular primary teethJ Indian Soc Pedod Prevent Dent 2009 27(2):108-10.10.4103/0970-4388.5533619736504 [Google Scholar] [CrossRef] [PubMed]
[12]. Hagman FT, Fused primary teeth: A documented familial report of caseASDC J Dent Child 1985 52(6):459-60. [Google Scholar]
[13]. Rajashekhara BS, Bhavana D, Manjunatha BS, Poonacha KS, Sunanda G Sujan, Bilateral fusion of primary mandibular lateral incisors and canines: A report of rare caseRevistaodontociencia 2010 25(4):427-29.10.1590/S1980-65232010000400020 [Google Scholar] [CrossRef]
[14]. Erdem GB, Uzamio M, Olmez S, Sagon MF, Primary incisor triplication defectJ Dent Child 2001 68(5-6):322-25.:301 [Google Scholar]
[15]. Neves AA, Neves ML, Farinhas JA, Bilateral connation of permanent mandibular incisors: A case reportInt J of Pediat Dent 2002 12(1):61-65.10.1046/j.0960-7439.2001.00324.x11858216 [Google Scholar] [CrossRef] [PubMed]
[16]. Cho SY, Primary Double Tooth: Report of a rare correlation with the permanent dentitionPrimary Dental Care 2007 14(2):48-50.10.1308/135576107780556734 [Google Scholar] [CrossRef]
[17]. Gellin ME, The distribution of anomalies of primary anterior teeth and their effect on the permanent successorsDent Clin North Am 1984 28(1):69-80. [Google Scholar]
[18]. Acharya AB, Taylor JA, Are a minimum number of condordant matches needed to establish identity in Forensic Odontology?Journal of Forensic Odonto-Stomatology 2003 21:6-13. [Google Scholar]