Dental plaque is an etiological factor for dental caries and periodontal diseases. The plaque control method both mechanical and chemical is an important component of oral health promotion [1,2]. Mechanical control is an important behaviour oriented measure to good oral hygiene, so toothbrushing for an effective plaque control program, depends on the technique used and ease of the performance. Many different toothbrushing techniques have been recommended over the past 20-30 years [3]. There are various methods (Bass method, Modified Bass method, Stillman’s method, Charters method, Scrub method etc.,) which are effective in removing plaque biofilm and debris, stimulate the gingiva, and deliver fluoridated dentifrice to the tooth surfaces [3].
No single method of tooth brushing is superior to the other. Patients usually employ their own methods of toothbrushing like vigorous scrubbing in horizontal, vertical or circular directions. Such techniques can successfully remove plaque but is very detrimental to the oral hard tissues [3]. To have any evidence based decision in this matter, the current evidence in literature on the efficacy of plaque removal by normal tooth brushing practices albeit performed with improvement must be reviewed. There is a lacuna of evidence or information on the effectiveness of any one method of toothbrushing. We designed this study to review all the randomised controlled trials that were reported on the efficacy of various manual toothbrushing techniques, in relation to their ability in the effective removal of plaque and maintainence of the health of the gingiva and periodontium.
Materials and Methods
Search Methods for Identification of Studies
For identification of the studies included in this review, we devised a search strategy for each database. The search strategy used a combination of meticulous vocabulary and free text terms. The main search databases (1950 till May 2017) were Medline via NCBI, Google scholar and Cochrane Central Register of Controlled Trials [Table/Fig-1].
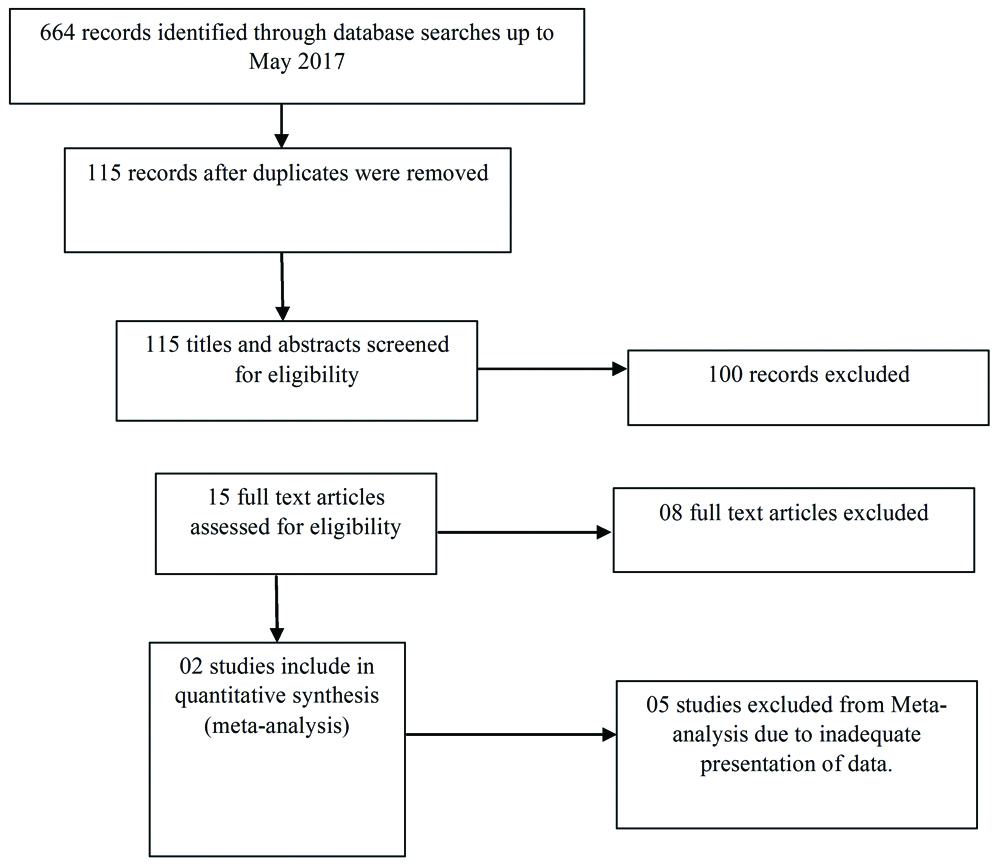
Flow chart of study selection in this update.
No restriction was placed on the language or date of the publication. The search terms used were: toothbrushing; toothbrushing techniques AND plaque removal; oral hygiene; oral hygiene AND gingivitis; oral hygiene AND plaque removal; plaque control; plaque control AND tooth brushing techniques; randomised controlled trials AND toothbrushing techniques AND plaque control; gingivitis AND toothbrushing techniques.
Type of studies: Randomised controlled trials comparing the different toothbrushing techniques were only included. Cross- over trials (with wash out period) and split mouth trials were also included in the study. Studies were included irrespective of the year of publication or language.
Type of participants: Those people who did not have any physical or mental disabilities were included. The age group of the trial participants was between 16-45 years. Individuals wearing orthodontic appliances were also included in the study.
Type of interventions: Different types of toothbrushing techniques were the interventions used. Studies with other interventions, in adjunct to the toothbrushing techniques, like the difference between manual and powered toothbrushes, use of other oral hygiene aids and effect of oral health education were not included. The studies that allowed the study participants to continue with the oral hygiene aids during the study were included in the review.
Outcome Measures
The outcome measures used were decrease in plaque scores or gingivitis scores or both, using the various plaque and gingival indices. When possible, the values obtained at the start of the study when the participants were enrolled in the study were used.
Data Collection and Analysis
Selection of Studies
Two authors Farheen Taha (FT) and Chandrashekar Janakiram (CJ) independently reviewed all the titles and abstracts of the studies for this review. If the study did not adequately meet the requirements of the review, it was considered as discarded. There was no disagreement between the authors in the selection of the studies. Once the studies were finalised, all the data was extracted in MS Excel using two well-known scales (Jadad scale and Risk of bias assessment scale of Cochrane Collaboration).
Jadad scale: In order to assess the methodological quality of included studies, Jadad scale was used. Initially 49 non-redundant items were present in the scale which later got reduced to 11 items due to poor face validity [4]. The authors (Farheen Taha and Chandrashekar Janakiram) have used all the 11 items in this review.
Data Extraction and Management
Piloting of data extraction was done by one of the authors (Farheen Taha). Both the authors (Farheen Taha and Chandrashekar Janakiram) agreed on the design of the data extraction form. The final data extraction protocol included the following information like bibliographic details of the study, clarity of the hypotheses and objective of the study, baseline characteristics of the participants in the study like age, gender of the participant, ethnicity of the participant, number of participants, criteria for selection of participants etc. In addition following characteristics like baseline scores, scores at subsequent follow-ups and outcomes including plaque and gingival indices, number of times the participants brushed their teeth, the type of toothbrush and toothpaste used, whether any toothbrushing technique was demonstrated to the patient and the presence of any other oral hygiene aids used in the studies, type of randomised controlled trial, design of randomised controlled trial and the method of randomisation, duration of the trial, frequency of assessment, and number of teeth assessed and the specific sites on the tooth assessed were included.
Measures of Treatment Effect
Mean difference and corresponding confidence interval of 95% was used for the estimation of effect. Many trials used different scales to measure the plaque, so Standard Mean Deviation (SMD), was used to estimate the treatment effect. The difference was estimated at baseline and post-intervention. In the two trials selected for meta-analysis, the baseline measurements were taken and later the follow up measurements were taken at three weeks.
Characteristics of Participants
Most of the study participants were adults; there were no notable medical histories to the patients. All the participants except in one study [5] were Caucasians. One trial [5] included orthodontic patients and one trial [6] included computer generated demonstration of the toothbrushing technique. Patients with periodontitis or any situation where the health of the periodontium was compromised were not included in the trials. All the seven trials had mostly adult participants. Two trials [5,7] recruited participants from dental schools/clinics, three trials [3,6,8] selected the study participants from university or secondary school students. None of the trials had school children as study participants.
One trial [6] detailed smoking as an exclusion criterion, two trials [3,8] did not include people with carious lesions, two trials [3,5] excluded participants with previous periodontal treatments, one trial [3] excluded participants on antibiotic therapy, two trials [3,8] did not undertake participants who had malocclusion, tooth malposition or crowding and one trial [7] was explicit that they will not recruit any members who had previous knowledge of the intervention brushing technique.
Characteristics of Interventions
The interventions included in the studies were the different tooth brushing techniques. Modified Bass technique was the most frequently used intervention [3,6,7]. The other techniques were the Fones technique, Bass technique, Roll technique, Scrub technique, Horizontal Scrub technique, Circular scrub, Charters technique and the Modified Stillman’s technique [Table/Fig-2] [5,6,8-10].
Summary of toothbrushing technique, number of trials and participants [3,5-10].
| Technique | Reference numbers | No. of trials | No. of participants in trials |
|---|
| Modified Bass technique | [3,6,7] | 03 | 211 |
| Fones technique | [6] | 01 | 67 |
| Bass technique | [5,8] | 02 | 90 |
| Horizontal scrub technique | [9,10] | 02 | 24 |
| Roll technique | [8,9] | 03 | 84 |
| Scrub technique | [8] | 01 | 60 |
| Circular scrub technique | [9] | 01 | 24 |
| Charters technique | [8,10] | 02 | 60 |
| Modified Stillman’s technique | [5] | 01 | 30 |
We assume, the type of the toothpaste was not relevant since most studies used the patients’ habitual toothpaste. The toothbrushes were manual standard toothbrushes, for matching and to prevent discrepancies. There was no mention of the toothpastes being fluoridated or not. The brushing techniques were demonstrated to each of the study subjects across all the studies. Various trials demonstrated the techniques differently. One study employed computerised-based demonstration [6], one study used a model and video presentation to demonstrate [3], one study had one of the investigators brushing the participant’s teeth [8] (prior to the trial, the investigators brushing the teeth were trained and standardised), other studies did not specify the method of demonstration. The type of dentifrice used and the number of times of brushing the teeth were not deliberated. These data were missing in the included studies.
Characteristics of Outcome Measures
Two trials [3,8] provided data for analysis on plaque and gingivitis at one to eight weeks and two trials [5,6] provided data for longer than eight weeks. If it was not stated that a full or partial mouth index was used, we assumed it was full mouth. Three trials [3,5,6] reported gingivitis data and five trials [3,5-8] reported plaque data. The following plaque and gingival indices were reported; Quigley Hein (Turesky) [3,6], Loe and Silness index [5], Silness and Loe index [5,8,10], Bergenholtz A et al., modification of Loe and Silness index [9] and Papillary bleeding index [6].
Excluded Studies
Many trials were ineligible for more than one reason; however, the primary reason for exclusion was the absence of the desired intervention. Trials with insufficient information and incomplete data were excluded.
Dealing with Missing Data
Whenever there was missing data, the trial authors of the respective study were contacted. Data remained excluded until clarification was obtained from the authors.
Data Synthesis
Fixed effect models were used for evaluation of the study. Data from cross-over trials were also used. The values and results of each study were represented separately.
Presentation of Primary Outcome
A ‘Summary of findings’ table was developed for the primary outcome of this review. [Table/Fig-3] provided adequate information regarding the general quality of the evidence from the trials, the magnitude of the effect of the interventions done and the data on primary outcomes [Table/Fig-3].
Summary of findings for the main comparison.
| Efficacy of plaque control by the various toothbrushing techniques (plaque index) |
|---|
| Studies | No. of participants | Bass group | Control group | p-value |
|---|
| Plaque index at baseline | Plaque index at follow-up | Plaque index at baseline | Plaque index at follow-up |
|---|
| Poyato FM et al., [3] | 46 | 3.19 (±0.57) | 1.62 (±0.36) | 3.11 (±0.54) | 2.60 (±0.54) | p<0.05 |
| Harnacke D et al., [6] | 56 | 2.50 (±0.49) | 1.97 (±0.54) | 2.57 (±0.56) | 1.86 (±0.52) | p=0.182 |
| Adverse events | There was no relationship seen between the different toothbrushing technique and soft tissue or hard tissue trauma. This may be due to very sparingly reported adverse effects or outcomes across the trials selected for the review. |
Subgroup Analysis and Investigation of Heterogeneity
Subgroup analyses and investigation of heterogeneity was not undertaken to examine the effects of concealed allocation, randomisation and blinded outcome assessment on the overall estimates of effect for important outcomes.
Meta-Analysis Methods
The basis of meta-analyses was the published means and SD for the plaque removing efficacy of modified bass technique with other toothbrushing techniques. Heterogeneity of study specific effects was assessed using I2 statistics. Random effects and fixed effect models were calculated. Indication of heterogeneity was also assessed using the Review Manager (RevMan). A forest plot using RevMan software [11] was used to display the results of the meta-analysis.
Results
Initially through PubMed and later through other search engines like Cochrane Central Register of Controlled Trials and Google scholar, 664 articles were identified up till May 2017. From that 115 remained after duplicates were removed. These 115 titles and abstracts were screened for eligibility and a further 100 were removed since they were not conforming to the essence of this review and were not contributing any significant data. Further 15 full text article [3,5-10,12-19] were screened for eligibility and eight articles were removed based on the eligibility criteria. The remaining seven studies [3,5-10] from five publications were included. Data was extracted from these final studies using the risk of assessment bias and Jadad Scale. These seven studies adequately met the eligibility criteria. Meta-analysis was done on two studies since only these studies provided adequate data for meta-analysis [3,6].
Included Studies
Of the seven included studies, two were conducted in Giessen, Germany [6,7]. One each in Sweden [9], Norway [10], Brazil [5], Spain [3] and United States of America [8]. The articles were published between 1970 and 2013. Two were published in the 1970s, one in 1984 and the rest four in 2003, 2009, 2012 and 2013. The combined total number of participants included across all the trials was 314. The number of subjects who were lost to follow-up was not specified in most of the studies.
Risk of Bias in Included Studies
All the seven studies [3,5-10], including the ones not considered for meta-analysis were assessed for risk of bias [Table/Fig-4]. Overall, two were deemed as low risk of bias [6,7] and the other five studies [3,5,8-10] were seen as of high risk of bias.
Risk of bias graph: review author’s judgement about each risk of bias item presented as percentages across all included studies.

Allocation
The generation of randomisation sequence was at low risk of bias for two trials (28.5%), unclear risk for two trials (28.5%) and high risk of bias (43%). The concealment of allocation was at low risk of bias for two trials (28.5%), unclear risk of bias for three trials (44%) and high risk of bias for two trials (28.5%).
Blinding
The outcome assessment was a low risk of bias for majority of the trials which were five trials (71%), and one trial each as unclear risk of bias and high risk of bias.
Incomplete Outcome Data
Of the seven studies included in the review, the attrition rates were specified in two studies. The dropout rate ranged from 16% to 21%. In the remaining five studies (although the exact reason for attrition was not clear), there was a mention of the number of subjects at the end of the study. In them, the attrition was 32 out of the total of 325 subjects (9.8%). Three studies (48%) were at low risk of bias in relation to incomplete outcome data with attrition rate and exclusion rate [3,5,6]. Two studies were of unclear risk and high risk each [8,10].
Selective Reporting
It is imperative to note that, the trial protocols could not be obtained. However, all the trials included in the review reported pre-specified and vital outcomes.
Other Potential Sources of Bias
All the trials were assessed as of being at low risk of bias because all the relevant details were present. No confounders were evident, and the trial authors had taken care of any possible bias. Even the Hawthorne bias was specifically mentioned in most trials.
Primary Outcomes
Plaque: There were five studies that measured plaque scores among the participants. One study indicated that the Modified Bass technique was superior to the normal brushing technique adopted by the patient [3]. Another study [6] compared Modified Bass, Fones and regular toothbrushing technique which was horizontal scrub technique. This study showed that the Fones technique was the most superior. However, modified Bass technique came a close second and was undeniably more efficient in plaque removal compared to the horizontal scrub technique. One other study showed that the Bass technique was more superior to the Stillman’s technique and scrub technique in plaque removal [5].
The remaining two trials included in the review where the plaque index was used, and the plaque level assessed, did not have any plaque scores/values cited in the article and the trial authors could not be contacted as no corresponding details were provided in the article [8,10].
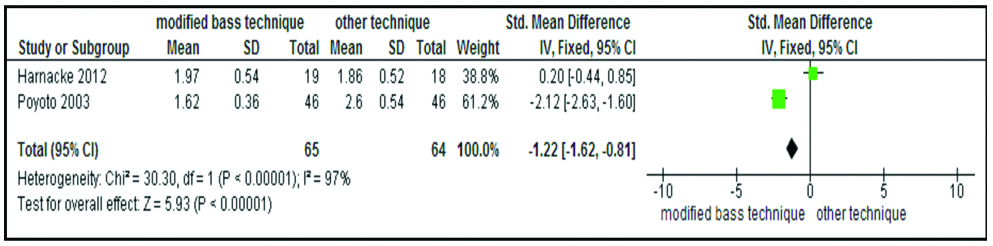
Finally, meta-analysis was attempted on two trials [3,6]. The characteristics of which are enumerated in [Table/Fig-5]. Both the trials were comparing modified Bass technique with routine technique. The quantitative analysis was significant with a 95% Confidence Interval of -1.22 (-1.62, -0.81). Chi-square value of 30.30, p<0.00001 and I2=97%. The meta-analysis revealed that the modified Bass technique was a better toothbrushing technique in terms of efficient plaque removal [Table/Fig-6].
Characteristics of studies included in the meta-analysis (Poyato FM 2003 and Harnacke D 2012) [3,6].
| Poyato FM 2003 |
|---|
| Methods | Clinical trial, cross-over, single blind, 6 weeks, n=46 (10 males and 36 females. |
| Participants | Caucasians, Spain, students, 18-30 years, periodontal pocket <4 mm, Ramjford calculus index <0.3, no medical problems. |
| Interventions | Modified Bass technique, twice daily, standard toothpaste (lacer) and toothbrush, no other oral hygiene aids used. |
| Outcomes | Turesky modification of Quigley Hein index. 2 days, 1 and 3 weeks. |
| Notes | Prior to each experiment, thorough prophylaxis to remove plaque, calculus and stains were given. |
| Harnacke D 2012 |
| Methods | RCT, stratified, parallel, single blind, 28 weeks, n=67, with 11 drop-outs. |
| Participants | Caucasians, Giessen-Germany, students, minimum 20 teeth, ≤10 showing plaque or bleeding, no smoking, no study of dentistry, no electrical toothbrushing. |
| Interventions | PowerPoint based training of modified Bass technique and Fones technique. Dental floss used. Elmex toothpaste and toothbrush. |
| Outcomes | Papillary bleeding index and Quigley and Hein index at full mouth sites. |
| Notes | Participants were given monetary compensation of (€ 50) and gift of oral hygiene products. |
Forest plot obtained by the meta-analysis of two studies included in the review.
Gingivitis: Three trials assessed gingivitis. Two of the three trials also checked for the plaque levels. In one of the studies [9], the participants developed gingivitis interproximally after a two week period of unsupervised brushing with their normal technique confirming the necessity of interdental cleaning. Study by Nassar PO et al., showed a very significant reduction percentage of gingivitis in the group that performed the Bass technique (13.6%) [5].
Secondary Outcomes
Calculus and stains: No trials reported on the difference in the degree of staining or any variation in the presence or absence of calculus on the tooth surface depending on the brushing technique employed.
Adherence: Only one trial [6] reported problems with adherence based on the ease and practicality of the brushing technique. The reasons of non-adherence were varied. Three participants reported unpleasant feeling (‘unfriendly to the gingiva’) as the main reason for non-adherence.
Adverse effects-soft tissue or hard tissue trauma: None of the studies cited any trauma or other adverse effects due to the toothbrushing technique.
Discussion
Summary of Primary Outcome
This review included seven studies where the effectiveness of different toothbrushing techniques in terms of plaque removal was established. In the present review, most trials selected were of short duration and had limited evidence as to the efficacy of the toothbrushing technique being studied. A recent report on toothbrushing techniques also observed that most trials assessing the efficacy of plaque control by the various toothbrushing techniques, involved a small number of participants, with a short follow-up, and varying levels of bias [20]. Furthermore, in our review, the lack of uniformity in the indices used to measure plaque and gingivitis, study duration and the interpretation of the evidence made pooling of the results difficult. Only one study [3] gave a clear indication where the modified Bass technique was significantly (p<0.05) more effective in removing supragingival plaque than the normal toothbrushing practice on all the sites. Another study by Nassar PO et al., done on patients with fixed orthodontic appliance showed that the Bass technique was more effective in reducing the periodontal clinical parameters of Plaque Index and Gingival Index [5].
Although most trials gave evidence in support of the Bass or modified Bass technique, one study by Harnacke D et al., indicated that the Fones technique was more adept at plaque control than the modified Bass technique [6]. But this needs to be contemplated since the author says that the external validity of the trial was in doubt since the study participants were university students, the male: female ratio was skewed, and it was a computer-based training of the toothbrushing technique. We also believe that the Fones technique yielded better results in the trial, because the Fones technique was taught since childhood and thus, they were on familiar grounds.
Meta-analysis done on the two trials; namely Poyato FM et al. and Harnacke D et al., presented that the modified Bass technique was more capable of removing plaque than the normal toothbrushing techniques (scrub technique), adopted by the participants [3,6]. In summary, the key learning from this review in terms of the efficacy of plaque control by the various toothbrushing techniques is very limited. The included studies were multifarious in terms of intervention duration, uniformity of examination and clinical outcomes. Consequently, it is difficult to give any clear evidence-based recommendations as to the best intervention designs with respect to efficient plaque control.
Overall Completeness and Applicability of Evidence
To our knowledge, this is probably the first systematic review that has attempted to assess the plaque removing efficacy of the various toothbrushing techniques. Although it is a known fact that toothbrushing is a very important plaque control measure [21], there was a dearth of knowledge on which toothbrushing technique to adopt. Albeit, the relationship between incomplete plaque removal, the squeal of gingivitis and periodontitis; and also the occurrence of dental caries has been proven [22]. There was a wide diversity between recommendations on toothbrushing methods, how often people should brush their teeth and for how long [20]. The wide diversity in recommendations should be a matter of concern for the dental professionals and dental regulatory bodies. Toothbrushing is the cornerstone of dental health education to prevent caries and periodontal disease and the fact that there is very little agreement on such a basic hygiene procedure has to be addressed [20].
In this review, the interventions done in the selected trials were subject to high levels of heterogeneity and ways of measuring the plaque outcomes varied. Meta-analysis could be conducted only on two studies. Additionally, subgroup analysis could not be conducted due to vast heterogeneity. More high quality and long-term studies are required to investigate the effectiveness of the brushing techniques in the treatment and prevention of gingivitis and periodontitis.
In the study by Poyato FM et al., the modified Bass technique is more efficient in terms of removing supragingival plaque from the lingual surface which is not the case in other toothbrushing techniques. Clinical practice also shows that patients pay poor attention to the lingual sites during their regular toothbrushing practices, probably because these sites do not affect the aesthetics and have more difficult access [3]. Certain factors may influence the effectiveness of the toothbrushing technique like the dexterity of the patient, level of comprehension of the patient after demonstrating the technique, the features of the toothbrush including filament arrangement, orientation, size, shape and flexibility. But all of them could not be isolated and analysed.
The Hawthorne effect i.e., the positive change in the behaviour of a subject as a result of the special attention and status received from participation in an investigation [23] has affected most studies and the trial authors have mentioned it. There is clear indication that the Hawthorne bias has the potential for profound prejudices [23] and hence, it should be taken care of. Publication bias was not very evident in any of the trials. It should be noted that, during the review, no methods were employed for detecting publication bias in any of the trials.
Quality of the Evidence
This systematic review and meta-analysis focused purely on randomised controlled trials. One trial (14%) was assessed as at low risk of bias, one at unclear risk of bias (14%) and five at high risk of bias (72%). Only two trials could be used in the meta-analysis; of which one was of unclear risk of bias and two were of high risk of bias. These trials were unable to demonstrate any statistically significant difference between any toothbrushing techniques. Although the effect estimates of plaque and gingivitis were slightly higher for the modified Bass/Bass technique in most trials. There was considerable heterogeneity in the meta-analysis for plaque and gingivitis for the analysis of the various toothbrushing techniques and for the meta-analysis of individual modes of action. This heterogeneity could not be explained.
Consequences of Clinical Practice/Research
Trials of longer duration are essential to completely understand the significant plaque and gingivitis reduction in the Bass/modified Bass technique. Data on the long-term benefits of the Bass/modified Bass technique will be valuable and can be used in the assessment of other outcomes such as the adverse effects, patient convenience and in the prevention of periodontitis and dental caries. This review could identify discrepancies in the design of the trials included in the review and in some cases the data could not be included for this reason. Whilst some of the trials were conducted before the current emphasis on experimental design, even the recent trials lacked power calculations and had not been analysed on an intention to treat basis but rather on the per protocol basis.
Implications for Research
Although this trial was done in the quest to identify the most efficient toothbrushing technique and to come to a professional consensus on which method of toothbrushing to recommend universally by the dentists, dental associations and government bodies; the purpose of this trial could not be completely achieved. Indeed, the modified Bass/Bass technique has attained some significance, but it was very marginal.
Researchers involved in these trials would be advised to study guidance on the design and reporting of clinical trials such as that provided in the CONSORT statement [24]. Better follow-up intervals and the use of much more sensitive indices would benefit both trials and future meta-analyses.
Deinzer R et al., says that several plaque indices are available to assess the oral hygiene like the Turesky modification of Quigley and Hein index, Silness and Loe index, Modified navy plaque index, Axial and the proximal plaque extension index etc. But indices like the Turesky modification of the Quigley and Hein index (TQHI) do not allow the idiosyncratic analysis of plaque deposits although it is of high clinical significance with respect to gingivitis and periodontitis [25]. This could be another reason why a significant result could not be obtained while using a certain brushing technique since, most trials included in the meta-analysis had used the Turesky modification of the Quigley and Hein index.
Many studies did not have adequate data and values of the plaque levels were also missing. While in some studies, the sampling method employed, and the introduction of the intervention was also not accurate. Thus, these studies were excluded from the meta-analysis. Finally, empirical data on thresholds for clinically important differences in plaque and gingivitis levels would help to determine whether the toothbrushing techniques would provide important health benefits.
Limitation
Sensitivity and subgroup analysis could have been planned on the toothpaste (fluoridated/non-fluoridated) and on the type of toothbrush. However, it could not be done due to insufficient data and the presence of vast heterogeneity within the selected studies.
Conclusion
Implications for Practice
This review has found that, compared to all the prevalent toothbrushing techniques, modified Bass/Bass technique is the most effective in reducing plaque and gingivitis. Literature also suggests that, in some instances, by using the Bass technique the cleaning efficiency can reach a depth of 0.5 mm subgingivally. In some studies, the modified Stillman’s and Charter’s techniques have also shown some significance in plaque removal but they are variations of the Bass technique and are also designed to aid in the complete removal of plaque from the gingival margins. The reliability, compliance and adaptability of the technique were inconsistently reported. No side effects were reported in all the seven trials.