The anterior cruciate ligament reconstruction surgery is a very commonly performed orthopaedic procedure in the operation theatre on an outpatient basis [1]. This is attributed to the fact that it is one of the most often injured ligaments of the knee, affecting young, active individuals and females being at a 2-10-fold greater risk than males playing the same sport [2].
The facility to perform this surgery depends on effective postoperative pain control that ceases the need for overnight hospital stay [3]. Potent analgesia is crucial for full recovery of the knee [4], and reduction of postoperative morbidity [5]. The earlier the mobilisation, the better chance of prevention of arthrofibrosis [6-8].
Multimodal and pre-emptive analgesia protocols for knee surgeries have been effective in decreasing requirements for narcotic medications in the early postoperative period. The convenience of reducing the dose of intravenous narcotics lies in the fact that they are associated with a number of adverse effects such as nausea, vomiting, hypotension, respiratory depression, and constipation [9-13], which in turn can slow down rehabilitation [14].
The addition of a femoral nerve block to the analgesic regime offers better pain control [15] when compared to epidural or intravenous patient-controlled analgesia [4,16,17]. However, there is a small but clinically significant risk of patient fall [18] due to enhanced motor blockade provided by femoral nerve block [19] due to weakening of the quadriceps muscle [20].
Whereas, the adductor canal block, that is executed at the mid-thigh level to anaesthetise the distal part of femoral nerve [21], purely sensory, is becoming a popular alternative to femoral nerve block for knee surgeries [22]. Due to the distal location of the nerve, this block provides comparable analgesia while preserving muscle strength [21,23]. The advent of ultrasonography has facilitated the anaesthesia personnel to visualise both the nerve and needle, as well as the spread of the drug, which enhances the success rate of nerve blocks [24]. The present study had compared the adductor canal block versus the femoral nerve block, in terms of analgesic efficacy and preservation of muscle strength following anterior cruciate reconstruction surgery.
Materials and Methods
The prospective, randomised controlled trial was done after approval from Institutional Ethics Committee, Kasturba Medical College, Manipal Academy of Higher Education, Mangalore, Karnataka, India, in a tertiary care centre from October 2016 to June 2018. A total of 76 patients posted for elective surgeries of the anterior cruciate ligament were chosen using computer-generated block randomisation. It was a single-blinded study (CTRI registration number: CTRI/2018/01/011614) [Table/Fig-1].

Inclusion Criteria
To qualify for inclusion, patients had to be between the age of 18 to 60 years, ASA physical status Class 1 and 2, with a body mass index of <35 kg/m2.
The following patients were excluded from the study:
Those who refused to participate in the study, patients who were pregnant, having significant psychiatric or mental disorders, with a coagulopathy, local skin infection or an allergy to local anaesthetics.
The patients were divided into two groups:
Group A: Those receiving adductor canal block with 15 mL of 0.125% bupivacaine and 25 mcg fentanyl,
Group F: Those receiving femoral nerve block with 15 mL of 0.125% bupivacaine and 25 mcg fentanyl
All patients underwent detailed pre-anaesthetic evaluation.
The study protocol was explained to the patients and written informed consent was obtained. A fasting period of six hours prior to the surgery was advised. They were then shifted to the operating room. Monitors connected were electrocardiogram, pulse-oximetry and non-invasive blood pressure. An appropriate sized intravenous cannula was secured for drug and fluid administration.
Patients were pre-medicated with midazolam 0.02 mg/kg and fentanyl 2 mcg/kg.
Patients were induced with propofol 2 mg/kg and airway was secured using an appropriate sized supraglottic airway device. Intraoperatively, heart rate, non-invasive blood pressure, ECG and oxygen saturation were monitored every five minutes. Patients were maintained on O2:N2O at 1:1 and sevoflurane to maintain a MAC of 1 throughout the procedure. Thirty minutes before the case ended; ondansetron was given to prevent postoperative nausea and vomiting. Prior to extubation, the block was given to the patients depending on which group they have been allocated to, with the help of an ultrasound machine.
The supra-glottic airway device was removed once the patient was fully awake and taking adequate tidal volume and subsequently, the patient was shifted to the postoperative ward.
Primary Outcome
Postoperative pain relief: This was assessed using the following methods: Pain at 0, 12 and 24 hours post-surgery using VAS. Patients who complained of pain corresponding to a score of 3 or more at rest were given a rescue analgesic; injection diclofenac sodium 1 mg/kg in 100 mL NS over 10 to 15 minutes.
The postoperative time of first analgesic and total dose were recorded.
Secondary Outcome
Patient ambulation: This was assessed by measuring quadriceps function at 2, 12 and 24 hours post-surgery by comparing it with the opposite side using the Medical Research Council grading for muscle strength [Table/Fig-2].
Medical research council grading.
| Grade | Meaning |
|---|
| 0 | Complete paralysis |
| 1 | Flicker of contraction possible |
| 2 | Movement possible if gravity eliminated |
| 3 | Movement against gravity but not resistance |
| 4 | Movement possible against some resistance |
| 5 | Power normal (it is not normally possible to overcome a normal adult’s power) |
Ethics
The procedures followed were in accordance with the ethical standards of the Institutional Ethics Committee, Mangalore and with the Helsinki Declaration of 1975 that was revised in 2000.
Statistical Analysis
The sample size was calculated using the formula:

Where, Zα=1.96 (with 95% confidence interval)
Zβ=0.84 (with 80% power)The sample size was found to be 76. Data analysis was done using student unpaired t-test, student paired t-test, chi-square test, Fischer’s-exact test. Statistical Package for the Social Sciences (SPSS) version 17 was used. p<0.05 was considered as significant.
Results
Majority of patients in Group A were in the age group of 41-50 (42.9%), and those of Group F were in the age group of 41-50 (41.5%). This data was statistically non significant with a p-value of 0.682 [Table/Fig-3].
Age-wise division of patients.
| Age | Group A | Group F | Total |
|---|
| <30 years | 8 (22.9%) | 10 (24.4%) | 18 (23.7%) |
| 31-40 years | 8 (22.9%) | 6 (14.6%) | 14 (18.4%) |
| 41-50 years | 15 (42.9%) | 17 (41.5%) | 32 (42.1%) |
| >50 years | 4 (11.4%) | 8 (19.5%) | 12 (15.8%) |
| Total | 35 (100%) | 41 (100%) | 76 (100%) |
χ2=1.502, p=0.682, NS
In Group A, 54.3% of patients were females and 45.7% of patients were males. In Group F, 46.3% of patients were females and 53.7% were males. The gender distribution between the two groups was statistically non significant, with a p-value of 0.490 [Table/Fig-4].
Gender-wise distribution of patients.
| Sex | Group A | Group F | Total |
|---|
| Female | 19 (54.3%) | 19 (46.3%) | 38 (50.0%) |
| Male | 16 (45.7%) | 22 (53.7%) | 38 (50.0%) |
| Total | 35 (100%) | 41 (100%) | 76 (100%) |
χ2=0.477, p=0.490, NS
The ASA 1 group of patients, 85.7% belonged to Group A and 68.3% to Group F. From ASA 2 patients, 14.3% were in Group A and 31.7 to Group F. The disparity between the two groups was found to be statistically non significant with a p-value of 0.075 [Table/Fig-5].
The ASA status-wise distribution of patients.
| ASA | Group A | Group F | Total |
|---|
| 1 | 30 (85.7%) | 28 (68.3%) | 58 (76.3%) |
| 2 | 5 (14.3%) | 13 (31.7%) | 18 (23.7%) |
| Total | 35 (100%) | 41 (100%) | 76 (100%) |
χ2=3.171, p=0.075, NS
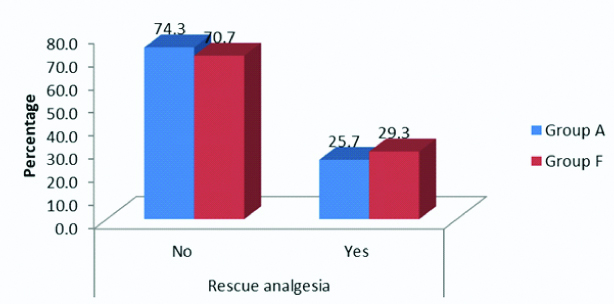
The incidence of requirement of rescue analgesia between the 2 groups showed that in Group A, 25.7% of the patients need edit, whereas rescue analgesia was required in 29.3% of the patients belonging to Group F. The difference between requirement of analgesics was statistically non significant (p=0.730) [Table/Fig-6].
Requirement of rescue analgesia between Group A and Group F.
Observing the differences in visual analogue scale score at 0 hours, 12 hours and 24 hours post block between both the groups showed that Group A had a visual analogue scale score of 2.29±1.447 at 0 hours, 3.26±1.669 at 12 hours and 3.86±1.7 at 24 hours, whereas Group F had a visual analogue scale score of 2.59±1.072 at 0 hours, 3.61±1.282 at 12 hours and 4.49±1.804 at 24 hours. The difference in visual analogue scale score between the two groups was statistically non significant [Table/Fig-7].
VAS score at 0,12 and 24 hours between Group A and Group F.

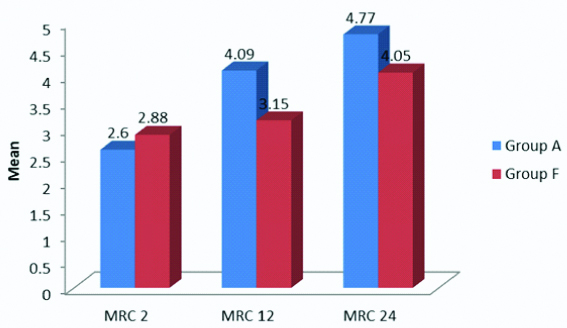
The Medical Research Council grading at two hours was 2.60±1.85 for Group A and 2.88±1.47 for Group F; not significant with a p-value of 0.468. At 12 hours, it was 4.09±1.011 for Group A and 3.15±1.216 for Group F; significant with a p-value of 0.001. At 24 hours, it was 4.77±0.646 for Group A and 4.05±1.341 for Group F; statistically significant with a p-value of 0.005 [Table/Fig-8].
MRC grading at 2, 12 and 24 hours between Group A and Group F.
Discussion
Authors conducted the present study to evaluate the motor sparing effect of adductor canal block versus femoral nerve block for arthroscopic anterior cruciate ligament reconstruction which was measured by the power of the lower limb with Medical Research Council Grading score following the block. The present results demonstrated that ACB spares quadriceps muscle strength compared to FNB. Patient satisfaction was however equal in both the groups which were measured using Visual Analogue Scale score.
There have been quite a few studies demonstrating the efficacy of adductor canal block in total knee arthroplasty [25], fewer in arthroscopic procedures, such as arthroscopic ligament reconstruction. Authors decided to restrict the present study to ACLR and include patient satisfaction score to the studied parameters.
The results of the present study concur with the study done by Kim DH et al., who performed a prospective double-blinded, randomised controlled trial in 2014, comparing adductor canal block with femoral nerve block in patients undergoing procedures of the knee [25]. They hypothesised that adductor canal block, compared with femoral nerve block, would exhibit less quadriceps weakness and demonstrate noninferior pain score and opioid consumption at 6-8 hours post-anaesthesia. They concluded that the adductor canal block, compared with the femoral nerve block, exhibited early relative sparing of quadriceps strength and was not inferior in providing analgesia or opioid intake.
Another study done in 2014, done by Chisholm MF et al., comparing both the blocks on adequate pain control following anterior cruciate ligament reconstruction [26]. They stated that there was no significant difference between the two groups in pain score and opioid consumption within postoperative 24-hours. However, they did not assess quadriceps muscle weakness in their study.
In 2013, a randomised controlled trial was done by Jaeger P et al., also demonstrated similar results [27]. The study concluded that femoral nerve block reduces motor strength by 49% whereas Adductor canal block reduces it only by 8%, which was not considered functionally important.
Kwesi Kwofie M et al., compared the two blocks in 2013 in a randomised controlled trial in terms of functional outcome but not in terms of analgesic potency [28]. They concluded that following femoral nerve block, there was a significant reduction in quadriceps strength and balance scores compared with baseline. There was no difference in hip adductor strength. However, in adductor canal block, the quadriceps strength and balance scores were similar to baseline.
In contrast, the study done by El Ahl MS, where adductor canal block was compared to femoral nerve block post anterior cruciate ligament reconstruction surgery showed that the patients who came under the adductor canal block group showed higher analgesic consumption, whereas the motor recovery was faster in the same [29]. the institution in which they had done the study used patellar tendon graft (as opposed to the traditional use of hamstring graft) which is supplied by the femoral nerve, and this could explain better analgesic outcome in the femoral nerve block group.
Limitation
There were a few limitations of the present study. A number of other factors which might have had an influence on the requirement of rescue analgesia, such as age and gender, experience of the operating surgeon and the anaesthesiologist administering the block. These factors were not compared in the present study. Another shortcoming was that physiotherapists in the present institution do not assess ambulation on the day of surgery. It is on postoperative day one, patients are encouraged to ambulate with assistance.
Conclusion
Based on the results, authors conclude that the adductor canal block is superior as an analgesic modality when compared to femoral nerve block because it provides pain relief just as much as femoral nerve block does, but it recoups the quadriceps motor power within 12-hours post block as opposed to the femoral nerve block which takes twice as much time.
χ2=1.502, p=0.682, NS
χ2=0.477, p=0.490, NS
χ2=3.171, p=0.075, NS