The Self-Directed Learning (SDL) is a skill which enables student to take initiative and responsibility of their learning by actively participating in the selection, management and assessment of own learning activities. Readiness to SDL can be measured and it suggests the level to which the person possesses the attributes required for enabling him to be a self-directed learner [1]. Due to constantly expanding medical knowledge database, medical professional must possess SDL skills which are precursor for lifelong learning attitude to maintain their professional competence [2]. Many active learning strategies including problem-based learning, Cooperative learning, E-learning, etc. have been suggested to improve SDL skills of the medical students, however these methods are not very cost-effective due to requirement of additional faculties, adequate learning spaces and for implementation of E-learning, adequate computer labs installed with costly E-learning software [3].
Limited data is available regarding the impact of an E-learning activity on SDL behaviour of students. Idrosa SN et al., evaluated the effect of E-learning module i.e., e-Student Oriented Learning Management System (e-SOLMS) on 239 Malaysian student’s SDL skills using SDL Readiness Scale (SDLRS) of Guglielmino and found that there was improvement in the SDL skills of students [4]. However, the study required costly E-learning software. Hence, the present study was conducted for evaluating the effect of E-learning module on student’s SDL behaviour prepared by using readily available computer tools such as Microsoft PowerPoint and assessed by SDLRS validated specially for medical students with the aim to assess the impact of E-learning activity on SDL readiness among second year MBBS students and to know the perception of students about the activity on antimicrobials (topic chosen for the study).
Materials and Methods
The single group pre-test/post-test experimental study was conducted at Andaman and Nicobar Islands Institute of Medical Sciences, Port Blair. Data from second year fifth semester MBBS students were collected before and after the intervention. The study was conducted after obtaining approval from Institutional Ethics Committee (Reg. NO.ECR/940/Inst/AN/2017). The study was conducted in August 2019.
Design: Convenience sample of 92 second MBBS fifth semester students were selected after obtaining informed consent from them. Initially, all students were requested to attend a special one hour contact session to explain them about the research project methodology. Total 87 students submitted their details (name, roll number, mobile number and email ID) to the principal investigator and were included in the analysis. Communication details were collected to give website access to the registered students. SDLRS developed by Hendry GD and Ginns P was administered to measure baseline data about SDL readiness [5].
After the pretesting, in an informal discussion, students were asked to suggest the topic for E-learning activity in Pharmacology. Majority of the students suggested to include topics from antimicrobial Pharmacology for the E-learning activity. Hence, E-learning module in the form of 6 interactive power-point presentations i.e., on antimicrobial pharmacology was prepared and uploaded on the website [Table/Fig-1].
Schematic Presentation of E-learning activity on Antimicrobial Pharmacology.
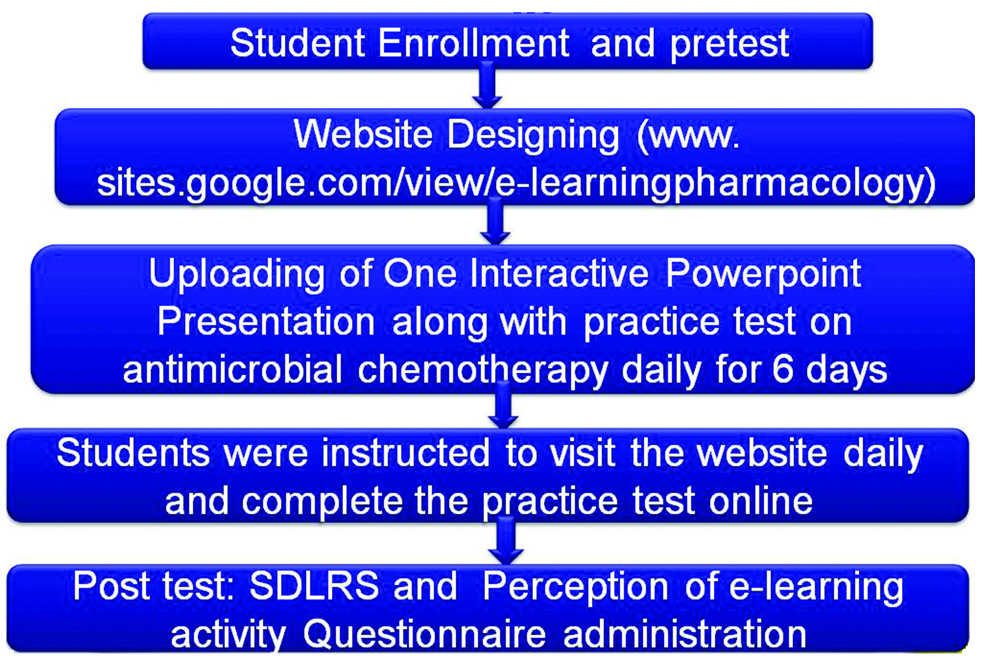
E-learning module: All PowerPoint Presentations were prepared using Microsoft Office PowerPoint 2007. All presentations included the learning objectives, previously validated by the subject expert in pharmacology, and only validated interactive Powerpoint presentations on six topics viz., sulfonamides, penicillins, cephalosporins, fluoroquinolones, macrolides and tetracyclines were uploaded on the website. All presentations were made interactive by inserting a multiple choice question slide after every two or three slides. The presentation was set up to run in a Kiosk mode in which computer mouse or laptop touchpad cannot be used to advance the slide. Instead hyperlinked pictures of “next slide”, “previous slide” and “home” were included for navigation through the presentation. On the MCQ slide only two hyperlinked pictures “previous slide” and “home” were inserted in such a way that the slide will advance to next section only after clicking the correct answer and user cannot advance directly to next slide. In case of doubt, a student can go back and again check previous section to successfully answer the question. All presentations were saved in PPSX file format which make the presentation non editable and directly opens in slide show mode after opening.
Website creation: Using freely available online tools such as Google sites, a website www.sites.google.com/view/e-learningpharmacology was created. One interactive PowerPoint presentation and one additional practice question set were uploaded daily, for six days. The additional practice set was created using Google Form which is free to use. Total six PowerPoint presentations and six additional practical question sets were uploaded.
E-learning session: During this, students were instructed to visit the above website daily and to complete the additional practice set given along with the presentation. Only participant students were given access to download the presentations. Students were asked to use either books, internet or discuss among their friends to answer the practice set or multiple-choice questions embedded in the PowerPoint presentations.
Post-test: Second contact session was conducted after one week of pre-test. In this session, revised SDLRS and E-learning activity perception questionnaire was administered.
Instruments: In this study, Revised SDLRS containing 35 items scale developed by Hendry G and Ginns P was used to measure students SDLR [5]. The revised SDLRs has 35 items instead of 42; a total SDLR score of >125 is considered as an indication for the readiness for SDL.
This instrument consists of 35 items measured on a 5-point Likert scale ranging from ‘Strongly Disagree’ to ‘Strongly Agree’. The scale is further categorised into following subscales:
Subscale 1: Critical Self Evaluation (CSE) consisting of 5 items.
Subscale 2: Learning Self Efficacy (LSE) consisting of 18 items.
Subscale 3: Self-Determination (SD) consisting of 4 items and
Subscale 4: Effective Organisation for Learning (EOL) consisting of 8 items.
Student’s Perception of E-learning activity Questionnaire having 6 items measured on a 5-point Likert scale ranging from ‘Strongly Disagree’ to ‘Strongly Agree’.
Statistical Analysis
The data were analysed using Statistical Package for Social Sciences (SPSS) Version 20. The categorical variables were described as median and interquartile range. Descriptive statistics was used to summarise demographic characteristics. As the revised SDLRS had 35 items instead of 42 items Fischer’s SDLR, a total SDLR score of >125 was considered as an indication for the readiness for SDL instead of score of >150. The comparison of scores of subscales and total SDLRS score was done by using Wilcoxon Signed Ranks Test. The p-value was considered significant at <0.05.
Results
Total 87 (52 female and 35 male) submitted the responses and were included in the analysis. The mean age of students was 18.16 with standard deviation of 0.3696.
[Table/Fig-2] shows comparison of SDLRS subscale and total scores between pre-test and post-test. The median total SDLR score in the post-test was 140 whereas in pre-test group it was 133. There was a statistically significant difference between total SDLRS scores (p<0.05) between the pre-test and post-test scores. Similarly, comparison of subscale scores revealed statistically significant difference in post-test scores of subscales i.e., CSE (p=0.007), LSE (p=0.003) and EOL (p=0.001) compared to pre-test scores.
Comparison of Achieved Self directed Learning (SDL) Readiness Scale Scores in pre-test and post-test.
| Subscales | Pre-test | Post-test | p-value |
|---|
| Mean±SD | Median | Mean±SD | Median |
|---|
| CSE | 18.84±2.710 | 19.00 | 19.93±3.019 | 20.00 | 0.007 |
| LSE | 71.06±7.109 | 72.00 | 73.98±7.693 | 75.00 | 0.003 |
| SD | 16.05±2.118 | 16.00 | 16.60±2.335 | 17.00 | 0.074 |
| EOL | 25.32±4.520 | 26.00 | 27.86±4.735 | 28.00 | 0.001 |
| Total SLDRS | 131.26±13.401 | 133.00 | 138.37±14.947 | 140.00 | <0.05* |
N=87, CSE: Critical self evaluation, LSE: Learning self efficacy, SD: Self-determination,
EOL: Effective organisation of learning, SD: Standard deviation; Wilcoxon signed ranks test used; *p <0.05 is considered as significant
The internal consistency for E-learning activity perception questionnaire was measured using Cronbach’s alpha and was found to be 0.736. Mode was observed to be four for five out of six items [Table/Fig-3].
Student’s Perception on E-learning Activity.
| Questions | SD | D | N | A | SA | Mode |
|---|
| Motivated me | 3 (3.4) | 6 (6.8) | 24 (27.5) | 39 (44.8) | 15 (17.24) | 4 |
| Enhanced my self learning | 1 (1.1) | 9 (10.3) | 24 (27.5) | 38 (43.6) | 15 (17.24) | 4 |
| Suits my learning style | 1 (1.1) | 10 (11.4) | 31 (35.6) | 34 (39.0) | 11 (12.6) | 4 |
| Could replace few lectures | 3 (3.4) | 17 (19.5) | 29 (33.3) | 24 (27.5) | 14 (16.0) | 3 |
| Can be incorporated in curriculum | 3 (3.4) | 9 (10.3) | 17 (19.5) | 36 (41.3) | 22 (25.28) | 4 |
| Recommended for other subjects | 1 (1.1) | 7 (8.0) | 14 (16.0) | 36 (41.3) | 29 (33.3) | 4 |
Values in parentheses indicate percentage; N=87; Likert scale: SD: Strongly disagree; D: Disagree; N: Neutral; A: Agree; SA: Strongly agree
Discussion
The present study was conducted with the objective of assessment of impact of E-learning activity on SDL readiness among second year MBBS students undergoing traditional curriculum and to know the perception of students about E-learning activity. The results of the study showed that when students were subjected to one week E-learning activity along with their routine teaching schedule, there is significant improvement in their SDL abilities as suggested by their total SDLR score as well as scores of subscales including CSE, LSE and EOL of revised SDLR scale. Although improvement seen in the SD subscale scores in post-test, however the difference was not statistically significant.
Baseline total SDLR score in measured in pre-test suggest that students had already strong tendency for SDL. Similar finding have been reported by Findley BW et al., in a study [6]. The probable reason for higher baseline SDLR score of >125 in pre-test may be due to clinical exposure from second year onwards of the course. Hence, apart from traditional didactic lecture based teaching, these students were also getting exposed to bedside teaching in the form of ward rounds, patient case presentations followed by discussions and also observations of clinician working in the wards, all creating an interest in students and thus improving their SDL skills [7].
Improvement in total SDLR as well as subscale scores can be explained on the basis of conceptual model proposed by Song L and Hill JR of E-learning which suggest that E-learning modules foster various SDL skills such as better utilisation of the resources to learn new information, designing of a strategy essential for effective organisation of learning including setting goals and time management, and self-reflection [8].
In a study by Svirko E et al., attitudes of 205 pre-clinical medical students towards computer aided learning course in neuoranatomy were evaluated using Revised Two-Factor Study Process Questionnaire (R-SPQ-2F) developed by Biggs and results of the study showed that it is necessary for a student to take control of their own learning pace, understand the E-learning module in better way, and evaluation of their own performance, which are all important attributes of SDL skills [9]. The interest created by the E-learning module for learning among students might be another reason for improvement of in SDLR scores seen after the E-learning activity in our study.
Improvement in the SDLR scores might also be due to interactive nature of PowerPoint presentations containing MCQ slide after every two or three slides as well as additional assignments given along with it might have resulted in fostering various important attributes of SDL skills such as the sense of responsibility for learning, the affection and enthusiasm for learning leading to better involvement of students in problem solving activities [10]. The non significant improvement in the SD subscale in post-test might be due the short duration of E-learning activity.
The E-learning activity was well perceived by the students as suggested by their scores on E-learning activity perception scale. Similar results have been reported in earlier studies [11,12]. As presentations were downloadable and no special software was required to run them, many students put these presentations on the pen drive and studied along with their friends. Such type of activity can provide ample opportunities for the development of social skills like collaboration, cooperation and consensus-making which are very essential for development of SDL skills.
Limitation(s)
This is a single group study design using a convenience sampling method. Better study design in future studies will further support the findings in the present study. The E-learning activity was conducted only for one week. Future studies should focus on analysing the effect of E-learning activities of longer duration on student’s performance. The effect of blended teaching learning methods i.e., traditional teaching learning coupled with self-directed E-learning activities on the academic performance is not estimated in this study. Future studies can be planned for estimation of cognitive gain using blended learning approaches. Basic computer literacy is mandatory for preparation of interactive PowerPoint presentations as well as for involvement in E-learning activity.
Conclusion(s)
In conclusion, the result of the study showed that E-learning activity on antimicrobial Pharmacology was very effective in fostering the SDL skills among second year MBBS students. Also, E-learning activity was very well received by the students as many suggested to include such type of learning methods for other subjects as well. Moreover, simple PowerPoint presentations can be very easily transformed into interactive presentations using Microsoft PowerPoint tools and can be uploaded to a free website provided by Google for planning simple E-learning activity. There is no need to purchase costlier software available for planning E-learning activity. Instead, the E-learning activity used in the current study represents one of the most cost effective ways of using E-learning technology for fostering the SDL behaviour among medical students which will enable them to a lifelong learner.
N=87, CSE: Critical self evaluation, LSE: Learning self efficacy, SD: Self-determination,
EOL: Effective organisation of learning, SD: Standard deviation; Wilcoxon signed ranks test used; *p <0.05 is considered as significant
Values in parentheses indicate percentage; N=87; Likert scale: SD: Strongly disagree; D: Disagree; N: Neutral; A: Agree; SA: Strongly agree