Bone Marrow Clot Section a Useful Tool for Diagnosis of Haematological Diseases- A Case Series
Parul Garg1, Harjot Kaur2, Ishwer Tayal3, Aradhana Singh Hada4
1 Assistant Professor, Department of Pathology, GGS Medical College, Faridkot, Punjab, India.
2 Professor, Department of Pathology, SGRD Institute of Medical Sciences and Research, Amritsar, Punjab, India.
3 Assistant Professor, Department of Forensic Medicine and Toxicology, GGS Medical College, Faridkot, Punjab, India.
4 Junior Resident, Department of Pathology, GGS Medical College, Faridkot, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ishwer Tayal, H. No. 81, GGS Medical College Campus, Sadiq Road, Faridkot, Punjab, India.
E-mail: pathology_parul45@ggsmch.org
Bone marrow examination is required for diagnosis of various haematological disorders. It includes both neoplastic and non-neoplastic disorders. Usually, bone marrow examination includes Bone Marrow Aspiration (BMA), bone marrow biopsy and bone marrow imprints. Bone marrow clot sections can also be an adjuvant of bone marrow examination and these sections are prepared from the left-over blood after aspirate smears. An adequate bone marrow clot section can be valuable for diagnosis of various diseases, especially in cases in which the aspirate and core biopsy material are inadequate or non contributory or it can be an adjuvant procedure. Little has been published about usefulness of bone marrow clot section. Studies are going on to evaluate the role of bone marrow clot section as an adjuvant or a diagnostic tool. This study includes a series of three cases in which bone marrow clot section was a diagnostic tool.
Adjuvant, Blood disorders, Bone marrow examination
Introduction
Bone marrow examination is an important tool for diagnosis of various haematological disorders. It is useful in confirming the clinically suspected disease or helpful in making a diagnosis [1,2]. In routine practice, BMA, touch imprint cytology and trephine biopsy are done for bone marrow evaluation. Bone marrow aspirate clot section can also be included as one of the components of bone marrow studies. The left-over aspirated material after preparing bone marrow slides can be used for preparing clot [3]. The clot formed is fixed in 10% formalin solution. Further processing was carried out as routine histopathology specimens.
These clot sections may add additional diagnostic information or it can be diagnostic at times. In this case series, the authors have discussed three cases in which the bone marrow clot section helped in reaching a confirmed diagnosis.
Case Series
Case 1
A 50-year-old, chronic alcoholic male came to a tertiary care institute with complaint of mass coming out from anal canal since one year. Systemic examination showed that patient had grade 3 piles for which he was recommended for surgery. No relevant past history was present. The patient underwent routine investigations before surgery.
Investigations showed haemoglobin of 7.4 gm/dL, total leukocyte count was 2200/cumm, differential count being lymphocytes 55%, atypical lymphoid cells 5%, neutrophils was 38%, eosinophil 2% and platelet count was 1 lac/cumm. The peripheral blood smear showed dual group of cells exhibiting moderate degree of anisopoikilocytosis with presence of macrocytes, macro-ovalocytes, microcytic hypochromic cells and elliptocytes [Table/Fig-1a]. Because of pancytopenia in Peripheral Blood Film (PBF), the patient underwent bone marrow examination.
Bone Marrow Aspiration (BMA) and trephine biopsy were performed and clot sections were also prepared. The aspirate smears were hypercellular and showed erythroid hyperplasia with predominantly normoblastic maturation. Granulopoiesis was relatively depressed and adequate megakaryocytes [Table/Fig-1b]. A 500-cell differential count was unremarkable in aspirates. Trephine biopsy had findings in agreement with the aspiration. However, the clot section in addition showed multiple foci of blast cells [Table/Fig-1c,d]. The blasts were large cells with nucleus having irregular nuclear margins, coarse chromatin, inconspicuous nucleoli and mild to moderate amount of cytoplasm.
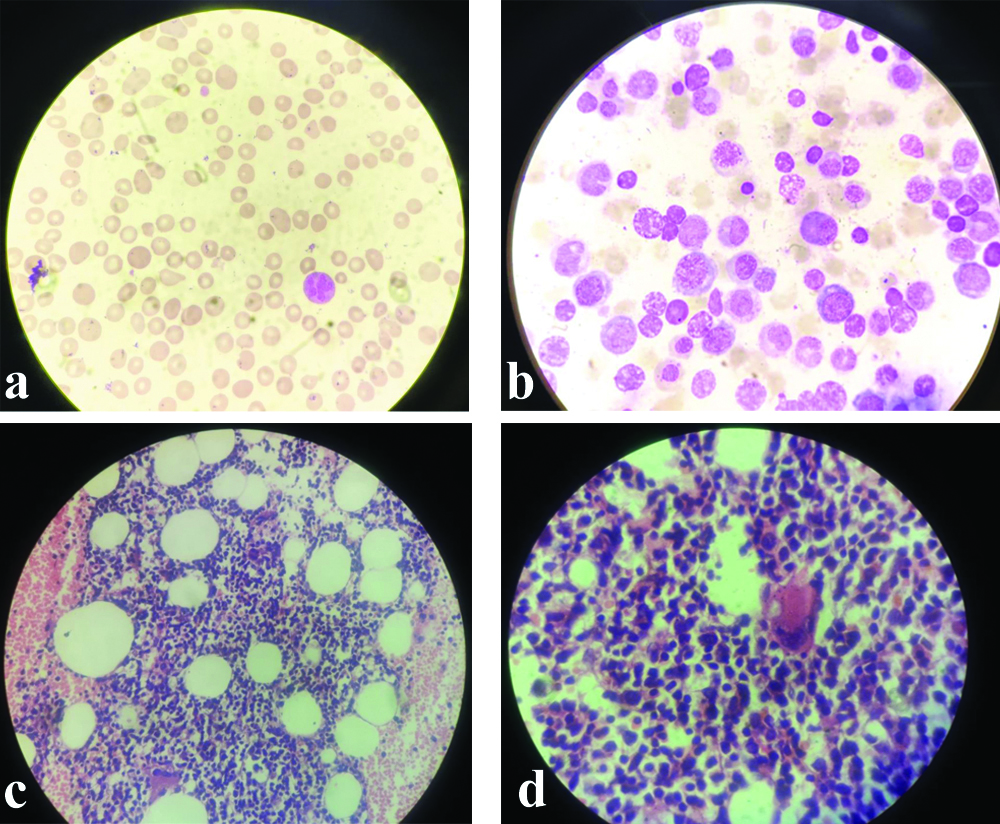
a) Peripheral blood film showing macrocytes macro-ovalocytes, microcytes and elliptical cell and tear drop cell. A hypersegmented neutrophil was also seen. (Leishman’s stain-400X); b) Bone marrow aspiration smears showing megaloblasts. (Leishman’s stain-100X); c) Bone marrow clot section showing nodule multiple foci, forming micronodule with blast cells. (H&E stain -400X): d) Bone marrow clot section showing nodule multiple foci, forming micronodule, with blast cells. (H&E stain -100X).
a) Peripheral blood film showing macrocytes macro-ovalocytes, microcytes and occasional tear drop cell. A hypersegmented neutrophil was also seen (Leishman’s stain-400X); b) Bone marrow clot section showing well-formed granuloma with langhan’s type of giant cell (H&E Stain -400X) c) Bone Marrow Aspiration (BMA) smear showing an ill formed granuloma. (Leishman’s stain-400X). This was found retrospectively when many granulomas were appreciated in bone marrow clot sections.

The aspirate and biopsy slides were re-evaluated by two different pathologists but the finding was same as earlier. Then the patient was re-evaluated for physical and systemic examination. But there was no organomegaly, lymphadenopathy or any other significant history except for bleeding from hemorrhoids. Patient complaint of weakness and some loss of weight for the past one month. Surgery was postponed. A repeat PBF was done after a period of five days. Repeat PBF shows similar picture like earlier except for differential counts. Blasts present in peripheral blood were 22%. These blasts were large cells with fine nuclear chromatin prominent 1 to 2 nucleoli and mild amount of cytoplasm. A diagnosis of acute myeloid leukaemia was given. The patient was referred to a higher centre for further management. Complete work-up was done there and the treatment was started. Patient was regularly followed but unfortunately the patient expired after four months.
Case 2
A 60-year-old male came for bone marrow examination with history of fever from past six months, he also had abdominal lymphadenopathy and splenomegaly. Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) for coronavirus was negative. The patient underwent bone marrow examination. PBF along with BMA and trephine biopsy were performed and clot sections were also prepared. But unfortunately, adequate biopsy specimen was not available. PBF showed mild degree of anisopoikilocytosis with presence of microcytic hypochromic cells, elliptical cells and macrocytes [Table/Fig-2a]. The aspirate smears were hypercellular and showed erythroid hyperplasia with micronormoblastic and megaloblastic maturation. Granulopoiesis showed orderly maturation and adequate megakaryocytes. A 500-cell differential count was unremarkable in aspirates. Trephine biopsy was very tiny, inadequate for comments. Examination of bone marrow clot showed necrotising granulomatous pathology [Table/Fig-2b]. Bone marrow aspirate slides were re-valuated and found occasional granulomas [Table/Fig-2c]. Patient was referred to pulmonary medicine department advised further investigations for tuberculosis. Patient was subjected to RT-PCR which showed positive results for tuberculosis and hence he was kept on antitubercular drugs.
Case 3
A 65-year-old male was diagnosed as a case of chronic lymphocytic leukaemia in 2016. The absolute lymphocyte count was 13200/cum [Table/Fig-3a]. In bone marrow, the lymphoid cells were 50% of all nucleated cells and bone marrow biopsy showed diffuse involvement of lymphoid cells [Table/Fig-3b-d]. He was on treatment since then. The patient was asked for a repeat bone marrow examination to look for morphological remission. BMA and biopsy along with clot section were done. PBF showed normocytic normochromic blood picture with normal total leukocyte count and differential counts within normal limits. BMA was normocellular with myelopoiesis showing orderly cell maturation and adequate megakaryocytes. Lymphocytes and lymphoid cells were within normal limits. Similar findings were seen in bone marrow biopsy. Clot section showed excess of lymphoid cells helping in diagnosis of presence of residual disease [Table/Fig-3e].
a) Peripheral blood film showing mature lymphocytes and smudge cell. (Leishman’s stain-400X) b) Bone Marrow Aspiration (BMA) smear showing increased lymphoid cells (Leishman’s stain-400X). c) Bone marrow biopsy showing diffuse involvement of lymphoid cells (H&E stain-100X). d) Bone marrow biopsy showing diffuse involvement of lymphoid cells (H&E stain-400X). e) Bone marrow clot section (which was prepared post treatment) showing collection of lymphoid cells (H&E stain -400X).

Discussion
Histopathological examination of paraffin embedded clot section is helpful in giving additional diagnostic information [4]. Sometimes these clot sections are helpful in reaching a diagnosis when the BMA is inadequate or bone marrow biopsy is inadequate or non-contributory [5]. In all the three cases, bone marrow aspirate and biopsy were non-diagnostic but the clot sections were helpful in diagnosis. Similar was the case reported by Kakkar N and Das S in which BMA and biopsy were non-diagnostic but clot showed a microfoci of plasma cells, showing the relapse of multiple myeloma [3]. Dee JW et al., also confirmed that in some cases clot sections are diagnostic of lymphoma whereas biopsy was negative [6]. Mathur K and Souter R reported that clot section was diagnostic in 75% cases of multiple myeloma [7]. Study done by Cantadori LO et al., confirms the validity of bone marrow biopsy for diagnosis [8]. Ong MG et al., concluded that cell blocks are superior to clot sections as clot sections have only sinusoidal blood [5]. Al-Diab JMA reported that 81% of the bone marrow clot section replaced the need for doing trephine biopsy but it was recommended that though there is good yield of bone marrow clot sections, it should be done complementary test along with trephine biopsy [9]. Farid J et al., also concluded that bone marrow clot section cannot replace bone marrow trephine biopsy, though there was no statistically significant difference between the results of trephine biopsy and marrow clot biopsy [10].
There are many advantages of bone marrow clot section over bone marrow biopsy. Bone marrow clot sections are easy to prepare, no decalcification is required, no separate invasive procedure is required and it allows the same kind of histological evaluation as bone marrow biopsy, except for the analysis of the architectural relationship between parenchyma/bone. So, some studies consider bone marrow aspirate clot (BMC) to be an alternative to bone marrow biopsy [5].
Clot sections can also be used for specialised procedures like immunohistochemistry. The clot sections have a better antigenic retrieval for immunohistochemistry as compared to bone marrow biopsy as decalcification is not required in clot sections. In-situ hybridisation studies also have shown better results with clot sections as compared with the conventional trephine biopsy [11]. Decalcification damages the nucleic acids and proteins which reduces the staining quality [9].
It has not been established whether clot section is an adjuvant or a diagnostic tool, whether it can replace bone marrow biopsy or not. Not much has been published about clot sections and its usefulness. This case series is an attempt to prove that clot sections can be used as a diagnostic tool.
Conclusion(s)
Bone marrow clot section not only provide additional information for diagnosis of the disease but it can be diagnostic when the BMA and biopsy failed to show any pathology. Similar was seen in this case series. These clot sections are very easy to prepare and no separate invasive procedure is needed for it. They are better than biopsy in case of immunohistochemistry and In situ hybridisation studies. However, it is difficult to interpret which case will be diagnosed by clot section and which will require biopsy. Hence, clot sections should be included and considered in every bone marrow examination.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Feb 18, 2021
Manual Googling: May 08, 2021
iThenticate Software: May 29, 2021 (9%)
[1]. Chandra S, Chandra H, Saini S, Bone marrow metastasis by solid tumors- Probable hematological indicators and comparison of bone marrow aspirate, touch imprint and trephine biopsyHematology 2010 15:368-72.10.1179/102453310X1264708362100120863433 [Google Scholar] [CrossRef] [PubMed]
[2]. Nanda A, Basu S, Marwaha N, Bone marrow trephine biopsy as an adjunct to bone marrow aspirationJ Assoc Physicians India 2002 50:893-95. [Google Scholar]
[3]. Kakkar N, Das S, Relapse of multiple myeloma: Diagnosis by clot section alone with negative bone marrow aspirate and trephine biopsyIndian J Pathol Microbiol 2009 52:290-91.10.4103/0377-4929.4895719332952 [Google Scholar] [CrossRef] [PubMed]
[4]. Barekman CL, Fair KP, Cotelingam D, Comparative utility of diagnostic bone-marrow components: A ten-year studyAm J Hematol 1997 56:37-41.10.1002/(SICI)1096-8652(199709)56:1<37::AID-AJH8>3.0.CO;2-3 [Google Scholar] [CrossRef]
[5]. Ong MG, Lowery-Nordberg M, Pillarisetti S, Veillon D, Cotelingam J, Maximizing the diagnostic yield from bone marrow aspirate material using the cell block technique on clot sectionsLab Med 2015 46:e24-27.10.1309/LM1FRVTIKXP3TDRT25829534 [Google Scholar] [CrossRef] [PubMed]
[6]. Dee JW, Valdivieso M, Drewinko B, Comparison of the efficacies of closed trephine needle biopsy, aspirated paraffin- Embedded clot sections, and smear preparation in the diagnosis of bone marrow involvement by lymphomaAm J Clin Pathol 1976 65:183-94.10.1093/ajcp/65.2.183766606 [Google Scholar] [CrossRef] [PubMed]
[7]. Mathur K, Souter R, The additional role of bone marrow particle sections (clot sections) in confirming marrow involvement by multiple myeloma: A single center studyInternational Journal of Laboratory Hematology 2010 32:e179-80.10.1111/j.1751-553X.2008.01136.x19196378 [Google Scholar] [CrossRef] [PubMed]
[8]. Cantadori LO, Gaiolla RD, Niero-Melo L, Oliveira CC, Bone marrow aspirate clot: A useful technique in diagnosis and follow-up of hematological disordersCase Reports in Hematology 2019 2019:759094810.1155/2019/759094830984433 [Google Scholar] [CrossRef] [PubMed]
[9]. Al-Diab JMA, Paraffin embedded marrow clot sections as an adjuvant procedure in the diagnosis of bone marrow diseasesMed J Basrah Univ 2016 34(1):15-19.10.33762/mjbu.2016.111183 [Google Scholar] [CrossRef]
[10]. Farid J, Idris M, Khan MA, Javed N, Moeen S, Role of bone marrow clot biopsy in workup of haematological and non-haematological diseasesMed Forum 2020 31(9):41-45. [Google Scholar]
[11]. Miranda RN, Mark HF, Medeiros LJ, Fluorescent in situ hybridisation in routinely processed bone marrow aspirate clot and core biopsy sectionsAm J Pathol 1994 145:1309-14. [Google Scholar]