Flabby ridges/displaceable tissues are a common finding in edentulous patients. Careful management is mandatory, failing which flabby ridges adversely affect the retention, stability and support of complete dentures. This article described a series of three clinical cases, which incorporated varied impression techniques and materials for recording this condition. Window technique with light body polyvinyl siloxane impression for maxillary ridge and double spacer with additional relief holes and light body polyvinylsiloxane impression for mandibular ridge were used for the first case, window technique with impression plaster for maxillary ridge was employed in the second case, and double spacer with additional relief holes and zinc oxide eugenol impression were used in the third case. From the conventional to the latest techniques utilised, the decision to consider which material is appropriate for a particular situation still remains in question. Moreover, the advent of newer dental materials also adds to this confusion. The proper diagnosis and planning is required for selecting the material and technique according to the displaceability of the tissues.
Complete denture, Hyperplastic tissue, Impression technique, Knife edged ridge
Introduction
A flabby ridge or fibrous ridge is a peripheral area where the soft tissue is mobile. It has been documented that excessive pressure, if applied over long and continuous periods of time on the edentulous ridges, alleviates bone resorption [1]. Flabby ridge is primarily seen in the maxillary anterior region and is usually correlated with characters of combination syndrome, as stated by Kelly E [2]. Previous studies showed that prevalence of flabby ridges varies in either arch, with 24% prevalence over maxilla and 5% in mandible [3,4]. Prosthodontic rehabilitation of compromised ridges in conventional manner is a cumbersome task. In order to fulfill the functional and aesthetic desires, customised treatment procedures must be considered. Flabby tissues, because of its resiliency, tend to get displaced while impression making and then return to its original form, thus displacing the denture [5]. This article discusses modified impression modalities for rehabilitation of three different patients with flabby ridges, who reported with the chief complaint of loose, ill-fitting dentures.
Case Series
Case 1
A 72-year-old male patient reported to the Department of Prosthodontics with the chief complaint of an ill-fitting complete denture since one year, which he had been wearing for 17 years [Table/Fig-1]. On intraoral examination maxillary anterior ridge had Grade 3 flabby tissue from canine to canine region [6] [Table/Fig-2a] and mandibular ridge extending from premolar to premolar region was knife edged with grade 1 degree of flabbiness [6] over the crest of ridge. Patient also had xerostomia [Table/Fig-2b]. Various treatment options such as surgical excision of flabby tissues followed by implant supported/retained prosthesis or complete denture fabrication using modified impression techniques were explained to the patient. Due to age factor and financial constraints, patient opted for complete denture using modified impression techniques for both maxillary and mandibular ridges.
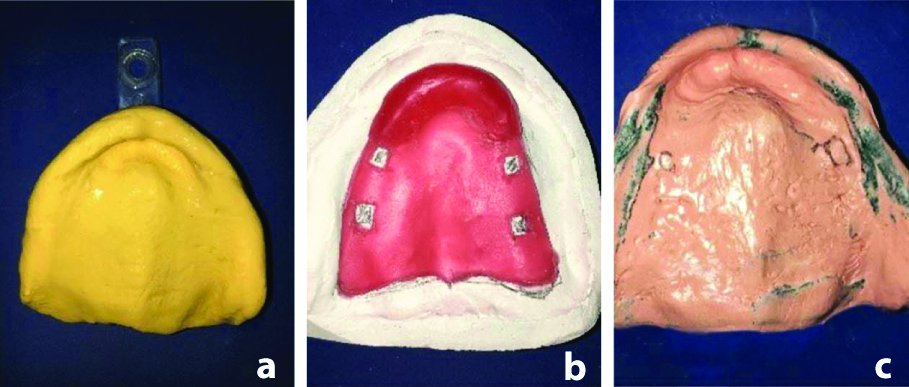
Since there was considerable displaceability of hyperplastic tissues, Window technique [7] for maxilla was decided. Double spacer technique for mandible was planned owing to the less significant flabby nature of the ridge. Flabby tissue over maxillary mandibular arches was marked with indelible pencil. Primary impressions were made with irreversible hydrocolloid and were poured with type 2 model plaster (La Jarden™ plaster of paris, Leo industries) to obtain diagnostic casts [Table/Fig-3a,b]. Complete coverage spacer, according to Boucher [8], was adapted with tissue stops on the maxillary cast. Custom tray was fabricated with self cure resin over the spacer with a handle placed palatally. Border moulding was done in maxillary arch with low fusing tray compound (DPI Pinnacle tracing sticks, Bombay trading corporation Ltd.) and wash impression was made with regular body reprosil hydrophilic vinyl polysiloxane impression material (Denstsply, Dentspro India Pvt. Ltd.) [Table/Fig-4a]. The impression was reseated on the ridge and the portion of the tray over the flabby ridge was cut out to form a window [Table/Fig-4b,c]. Light body material (GC, Flexceed putty and light body, GC India Dental) was then injected over the flabby tissue [Table/Fig-4d,e]. In the mandibular arch, special tray with double spacer was fabricated. Border moulding was done with low fusing tray compound (DPI Pinnacle tracing sticks, Bombay trading corporation Ltd.,) and then a wash impression was made with regular body reprosil hydrophilic vinyl polysiloxane impression material (Denstsply, Dentspro India Pvt. Ltd.) [Table/Fig-5a].
Case 1: Preoperative frontal view of the patient.
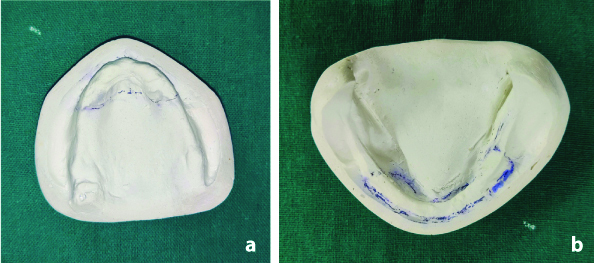
a) Case1: Intraoral view of maxilla (Flabby ridge portion marked by indelible pencil); b) Case1: Intraoral view of mandible (knife edge portion with slight amount of flabby tissue marked by indelible pencil).

a) Case 1: Poured maxillary diagnostic cast; b) Case 1: Poured mandibular diagnostic cast.
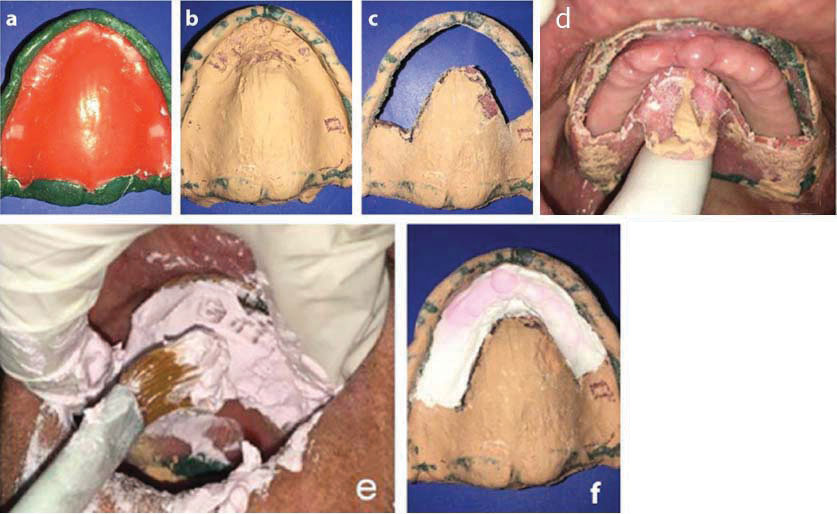
a) Case 1: Wash impression of maxillary arch made with regular body Reprosil Hydrophilic Vinyl Polysiloxane impression material; b) Case 1: A window was cut in the area corresponding to flabby ridge portion; c): Case 1: The tray with the cut window was tried in the patient’s mouth; d) Case 1: Light body Vinyl Polysiloxane impression material injected over the flabby tissue; e) Case 1: Completed maxillary impression.

a) Case 1: Mandibular wash impression made with regular body Reprosil hydrophilic Vinyl Polysiloxane impression material; b) Case 1: Area of mandibular knife edged ridge with flabby tissue region scraped off with No.23 BP blade and perforations made; c) Case 1: Completed mandibular impression.

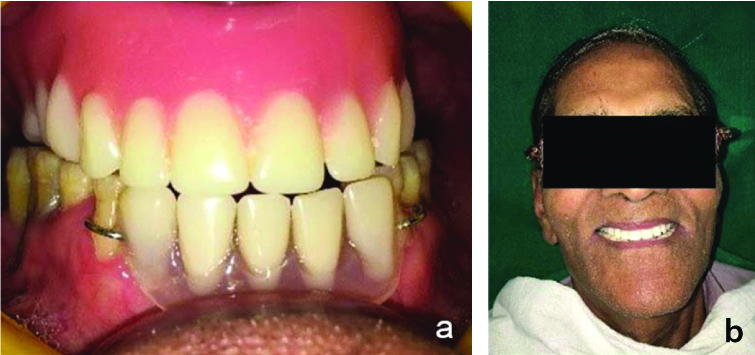
Area of flabby tissue region was scraped off with No.23 Bard Parker (BP) blade. Multiple perforations were made in the flabby portion [Table/Fig-5b] followed by a light body impression (GC Flexceed, GC India Dental [Table/Fig-5c]. Although zinc oxide eugenol offers minimum displaceability than addition silicone, latter was preferred as the impression material of choice in this case due to prevailing xerostomia condition of the patient. Then jaw relation was recorded, followed by wax trial and finally denture insertion [Table/Fig-6]. The patient was satisfied with the retentive and stable denture. Patient was advised to use salivary substitute (wet mouth) to enhance retention. No complications were reported in the subsequent recalls which were followed-up after two days, one week, one month and three months.
Case 1: Frontal view of the patient with inserted complete denture.

Case 2
A 75-year-old male patient came to the Department of Prosthodontics with the chief complaint of loose in complete denture since three months. Existing denture was fabricated 10-years-ago [Table/Fig-7]. Clinical examination revealed Grade 3 [6] flabby maxillary ridge from second premolar to second premolar region [Table/Fig-8] [6]. Here, conventional Window technique was planned due to the significant degree of flabbiness present [7]. Since, the mandibular ridge was not associated with any sort of pathology, a conventional mandibular denture was planned. Primary impression of maxillary and mandibular arch was made with irreversible hydrocolloid impression material (3M ESPE) [Table/Fig-9 a,b] and diagnostic cast was poured. A full spacer with tissue stops, as described by Boucher, was adapted onto the maxillary cast followed by a custom tray fabrication [8]. Border moulding of maxillary arch was performed with low fusing impression compound (DPI Pinnacle tracing sticks, Bombay trading corporation Ltd.) [Table/Fig-10 a] and wash impression was made with zinc oxide eugenol (Coltene, Coltene Whaledent Pvt. Ltd.) [Table/Fig-10b]. A window was cut out in the tray over the flabby ridge area [Table/Fig-10c,d]. Impression plaster (AFDRUK GIPS WT, Schouten Group) was painted over the flabby ridge in increments ensuring that the flabby ridge was not compressed and final impression was recorded [Table/Fig-10 e,f]. Border moulding of mandibular special tray was done using low fusing impression compound and wash impression was recorded using zinc oxide eugenol impression paste. Maxillary and mandibular master casts were poured from the impressions. The patient was satisfied with the fit of the final denture [Table/Fig-11]. At two days, one month and three months recall, patient turned up without any complications.
Case 2: Preoperative frontal view of the patient.
Case 2: Intraoral view of maxilla (Flabby ridge portion marked by indelible pencil).

Case 2 : a) Irreversible hydrocolloid impression of maxillary arch; b): Irreversible hydrocolloid impression of mandibular arch.

a) Case 2: Border moulding done on maxillary custom tray with conventional wax spacer; b) Case 2: Wash impression of maxillary arch made using Zinc Oxide Eugenol; c) Case 2: A window was cut in the area corresponding to flabby ridge portion; d) Case 2: The tray with the cut window was tried in the patient’s mouth; e) Case 2: Impression plaster painted over the flabby tissue; f) Case 2: Completed maxillary impression.
Case 2: Frontal view of the patient with inserted complete denture.

Case 3
A 71-year-old male reported to the Department of Prosthodontics with the chief complaint of an ill-fitting denture which was made seven years back [Table/Fig-12]. Intraoral examination revealed resorbed, completely edentulous maxillary ridge with Grade 1 classification of flabby tissues over the anterior region extending from canine to canine [6] [Table/Fig-13] and partially edentulous anterior region of the mandibular arch. Therefore, double spacer with multiple perforation impression technique was employed which offered minimal tissue distortion [9]. After the fabrication of primary cast from the obtained primary impression [Table/Fig-14a], double spacer (MAARC spacer wax, Shiva products) was adapted in the region of flabby tissue [Table/Fig-14b] and special tray was fabricated with clear self-cure acrylic (Pyrax acrylic self-cure, Pyraxpolymers, Rookee). After border moulding with low fusing tray compound (DPI Pinnacle tracing sticks, Bombay trading corporation Ltd.) spacer wax was removed and multiple vent holes were created over the marked areas of flabby ridge tissues. Wash impression was taken with zinc oxide eugenol impression paste (Coltene, Coltene Whaledent Pvt. Ltd.) [Table/Fig-14c]. Jaw relation and wax try in was done and followed by denture insertion [Table/Fig-15a,b]. Patient was comfortable with the delivered prosthesis. At periodic recalls, except for slight denture adjustments, patient reported no serious problems and didn’t have any complaints regarding the fit of the denture.
Case 3: Preoperative frontal view of the patient.

Case 3: Intraoral view of maxilla (flabby ridge portion marked by indelible pencil).

a) Case 3: Irreversible hydrocolloid impression of maxillary arch; b) Case 3: Maxillary preliminary cast with double spacer adapted; c) Case 3: Wash impression made using zinc oxide eugenol on border molded maxillary special tray.
a) Case 3: Inserted complete maxillary complete denture and mandibular removable partial denture; b) Case 3: Frontal view of the patient with inserted maxillary complete denture and mandibular removable partial denture.
Discussion
Surgical removal of fibrous tissues followed by prosthodontic rehabilitation is challenging and extensive. Stability and retention of the dentures can be improved by implant retained prosthesis. But the factors like financial constrains and duration of the procedure make it unsuitable for every patient. These all problems can be avoided by conventional prosthodontic treatment with some modifications in technique [9].
Such modifications have been described in literature as early as 1960’s with Liddlelow’s two part impression technique [10], with zinc oxide eugenol in the mucostatic areas and displaceable tissues with liquid plaster of paris. Osborne describes a palatal splinting using a two tray system [11], Watson’s Window technique [7], Fillers two tray technique [12], Zafrulla khans Window technique [13] are other commonly described techniques in the literature.
Of the various techniques, the controversy is which technique and which material to opt for. This can only be decided after careful diagnosis to determine the amount and position of the displaceable tissues. Massad J et al., has given a tooth in diagnosing and classifying flabby tissues. Massad J et al., ranked the displaceability of flabby tissue as attached, low mobility, low displacement; average, clinically acceptable; or high mobility, high displacement [6].
If the distortion of displaceable tissues is minimal, use of special tray with multiple perforations in the region of flabby tissue is sufficient. But if the distortion of displaceable tissues is significant, Watson’s window technique, Mc Cord and Grants technique, palatal splinting using two part tray system etc., [9] are employed.
In case 1, the maxillary flabby tissue was of Type III Massad classification [6], therefore materials of choice were either zinc oxide eugenol/regular body with plaster/light body with window technique. Since the patient was a moderate grade xerostomic Common Terminology Criteria for Adverse Events (CTCAE) grading scale [14] version 3.0) zinc oxide eugenol and plaster was avoided [15] and the impression made with regular body and light body. Adverse effects of zinc oxide eugenol in the oral cavity have been reported in accordance with its use in periodontal and surgical packs [16], root canal sealers [17,18] and certain mouth rinses [19] also. In case 1 mandible Massad grade 1 flabby tissue over the knife edged ridge was managed with double spacer and multiple perforations [9]. The sectioning and positioning of window was found sensitive and painting of the light body intraorally without dislodging the tray was challenging to an extent.
In case 2, grade of flabby tissue was falling under Massad Class III, zinc oxide eugenol with plaster was selected with window technique. Here the authors felt that the manipulation and application was cumbersome. In case 3, Massad grade 1 flabby tissue was only present and a simple double spacer technique was employed. It was noted that in all three cases displaceable tissue was located in the anterior region. It could probably be due to use of old ill fitting dentures, unplanned, uncontrolled extraction and load concentration on the anterior segment of the ridge such as anterior masticatory habits or anterior interference [2,20-22].
Conclusion(s)
Achieving stability and retention in fibrous ridges still remains a prosthodontic challenge even after the advent of surgical and implant retained treatment options. However, there is a lack of scientific evidence for support of any technique over the other. Treatment plan should be decided after determining the displaceability of the flabby tissues according to Massad classification and thereafter selecting the appropriate impression technique in the literature.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: May 08, 2021
Manual Googling: Sep 06, 2021
iThenticate Software: Sep 30, 2021 (7%)
[1]. Desjardins RP, Tolman DE, Etiology and management of hypermobile mucosa overlying the residual alveolar ridgeJ Prosthet Dent 1974 32(6):619-38.10.1016/0022-3913(74)90071-7 [Google Scholar] [CrossRef]
[2]. Kelly E, Changes caused by a mandibular removable partial denture opposing a maxillary complete dentureJ Prosthet Dent 1972 27(2):140-50.10.1016/0022-3913(72)90190-4 [Google Scholar] [CrossRef]
[3]. Allen PF, McCarthy S, Complete Dentures from Planning to Problem Solving 2003 London, UKQuintessence Publishing [Google Scholar]
[4]. Carlsson GE, Clinical morbidity and sequelae of treatment with complete denturesJ Prosthet Dent 1998 79(1):17-23.10.1016/S0022-3913(98)70188-X [Google Scholar] [CrossRef]
[5]. Collett HA, Complete denture impressionsJ Prosthet Dent 1965 15(4):603-14.10.1016/0022-3913(65)90030-2 [Google Scholar] [CrossRef]
[6]. Massad J, Lobel W, Garcia LT, Monarres A, Hammesfahr PD, Building the edentulous impression-a layering technique using multiple viscosities of impression materialCompend Contin Educ Dent 2006 27(8):446-51. [Google Scholar]
[7]. Jayaprakash MB, Sahu K, Khan M, Khoriya S, Jadhav S, Kendre B, Management of flabby ridge cases: A challenge in clinical practiceInt J Adv Health Sci 2014 1(5):32-37. [Google Scholar]
[8]. Jain AR, Dhanraj M, A clinical review of spacer design for conventional complete dentureBiol Med (Aligarh) 2016 8(5):0110.4172/0974-8369.1000307 [Google Scholar] [CrossRef]
[9]. Crawford RW, Walmsley AD, A review of prosthodontic management of fibrous ridgesBr Dent J 2005 199(11):715-19.10.1038/sj.bdj.481296816341179 [Google Scholar] [CrossRef] [PubMed]
[10]. Liddelow KP, The prosthetic treatment of the elderlyBr Dent J 1964 117(5):307-15. [Google Scholar]
[11]. Gomaa A, El Mekawy N, Impact of various impression techniques on maxillary flabby ridge tissue displacement (within-subject evaluation)Egyptian Dental Journal 2017 63(3):2681-89.10.21608/edj.2017.76228 [Google Scholar] [CrossRef]
[12]. Filler WH, Modified impression technique for hyperplastic alveolar ridgesJ Prosthet Dent 1971 25(6):609-12.10.1016/0022-3913(71)90122-3 [Google Scholar] [CrossRef]
[13]. Khan Z, Jaggers JH, Shay JS, Impressions of unsupported movable tissuesJ Am Dent Assoc 1981 103(4):590-92.10.14219/jada.archive.1981.02927026644 [Google Scholar] [CrossRef] [PubMed]
[14]. Minhas S, Kashif M, Altaf W, Afzal N, Nagi AH, Concomitant-chemoradiotherapy-associated oral lesions in patients with oral squamous-cell carcinomaCancer Biol Med 2017 14(2):176-82.10.20892/j.issn.2095-3941.2016.009628607808 [Google Scholar] [CrossRef] [PubMed]
[15]. Sarrami N, Pemberton MN, Thornhill MH, Theaker ED, Adverse reactions associated with the use of eugenol in dentistryBr Dent J 2002 193(5):257-59.10.1038/sj.bdj.480153912353045 [Google Scholar] [CrossRef] [PubMed]
[16]. Koch G, Magnusson B, Nyquist G, Contact allergy to medicaments and materials used in dentistry. II. Sensitivity to eugenol and colophonyOdontol Revy 1971 22(3):275-89. [Google Scholar]
[17]. Hensten-Pettersen A, Brstavik D, Wennberg A, Allergenic potential of root canal sealersDental Traumatology 1985 1(2):61-65.10.1111/j.1600-9657.1985.tb00562.x3861315 [Google Scholar] [CrossRef] [PubMed]
[18]. Barkin ME, Boyd JP, Cohen S, Acute allergic reaction to eugenolOral Surgery, Oral Medicine, Oral Pathology 1984 57(4):441-42.10.1016/0030-4220(84)90166-X [Google Scholar] [CrossRef]
[19]. Vilaplana J, Grimalt F, Romageura C, Conellana F, Contact dermatitis from eugenol in mouthwashContact Dermatitis 1991 24(3):223-24.10.1111/j.1600-0536.1991.tb01703.x1868706 [Google Scholar] [CrossRef] [PubMed]
[20]. Labban N, Management of the flabby ridge using a modified window technique and polyvinylsiloxane impression materialSaudi Dental Journal 2018 30(1):89-93.10.1016/j.sdentj.2017.10.00430166877 [Google Scholar] [CrossRef] [PubMed]
[21]. Chakarvarty K, Tomar SS, Tandan P, Modi R, Managing flabby tissue with different impression techniques: A case seriesIJOCR 2015 3:95-99. [Google Scholar]
[22]. Anne R, Manne P, Anne G, Muvva SB, Anche S, A simplified approach for management of flabby ridges-a case reportInternational Dental Journal of Students Research 2017 4:207-12.10.18231/2278-3784.2016.0007 [Google Scholar] [CrossRef]