Pelviureteric Junction Obstruction in Right Ectopic Pelvic Kidney and Left Blind Ureter: A Rare Case Report
Vilas Sabale1, Ashish Gavade2, Vikram Satav3
1 Professor, Department of Urology, Dr. D. Y. Patil Medical College, Hospital and Research Centre, Pimpri, Pune, Maharashtra, India.
2 Resident, Department of Urology, Dr. D. Y. Patil Medical College, Hospital and Research Centre, Pimpri, Pune, Maharashtra, India.
3 Professor, Department of Urology, Dr. D. Y. Patil Medical College, Hospital and Research Centre, Pimpri, Pune, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ashish Gavade, Resident, Department of Urology, Dr. D. Y. Patil Medical College, Hospital and Research Centre, Pimpri, Pune-411018, Maharashtra, India.
E-mail: ashishg0208@gmail.com
One in seven neonates on antenatal scan detected hydronephrosis has Pelviureteric Junction Obstruction (PUJO), making PUJO one of the most common cause of congenital urinary tract obstruction, with an incidence of one in 1000 to one in 2000 live births. Hereby, the authors present a case report of 19-year-old female who presented with pain in abdomen since, two weeks. There was no history of dysuria, haematuria. No history of lower urinary tract symptoms. No history of fever. There was no history of co-morbidity. No similar episodes of pain in past. All blood investigations were within normal limits with serum creatinine of 0.78 mg/dL. Computed Tomography (CT) Intravenous Urography (IVU) showed right ectopic kidney with Pelviureteric junction obstruction with left small atrophic kidney. Diethylenetriaminepentaacetic Acid (DTPA) reported crossed fused kidneys. Two investigations gave two different diagnoses. It made diagnosis and treatment challenging. Cystoscopy showed two ureteric orifices are normal position. Retrograde pyelogram showed left blind ureter. Right pelvic kidney was seen. Delayed drainage of contrast made diagnosis of pelvi ureteric junction obstruction. So it ruled out diagnosis of crossed fused kidneys with help of cystoscopy and retrograde pyelogram. Such anomalous kidneys are rare to find in day to day life. As anomalous kidneys usually have abnormal blood supply it makes surgery challenging. Abnormal position of kidney, malrotation makes surgery difficult. So decision was made to do open surgery for present patient. Open pyeloplasty was performed for right pelvi ureteric obstruction. Also, DTPA interpretation as anatomical investigation should be used with pinch of salt.
Congenital kidney disease, Pyeloplasty, Retrograde pyelography, Solitary functioning kidney
Case Report
A 19-year-old female came to the Urology Outpatient Department (OPD) for the first time with pain in abdomen since, two weeks. Pain was intermittent and was relieving on oral analgesics which patient took from outside hospital. There was no history of dysuria, haematuria. No history of lower urinary tract symptoms. No history of fever. There was no history of co-morbidity and no history of surgeries in past. No similar episodes of pain in past. Family history was insignificant. Initial differential diagnoses depending on history alone were stone disease, pelvi ureteric junction obstruction and cystic disease of kidney. The general physical examination was normal with the following vitals: pulse: 78/minute; blood pressure: 116/80 mmHg; afebrile and 98% SpO2 on room air. There was no icterus, clubbing, cyanosis, pallor, or lymphadenopathy. The systemic examination was normal. Local examination was normal. Laboratory reports were normal for the complete blood count, Liver Function Test (LFT), and blood glucose with normal renal function with normal serum creatinine level of 0.78. Computed Tomography (CT) report was suggestive of large right pelvic kidney of 13×6×7.5 cm with moderate hydronephrosis due to abrupt narrowing of PUJ as seen in [Table/Fig-1].
Coronal image of CT Intravenous Urography (IVU).
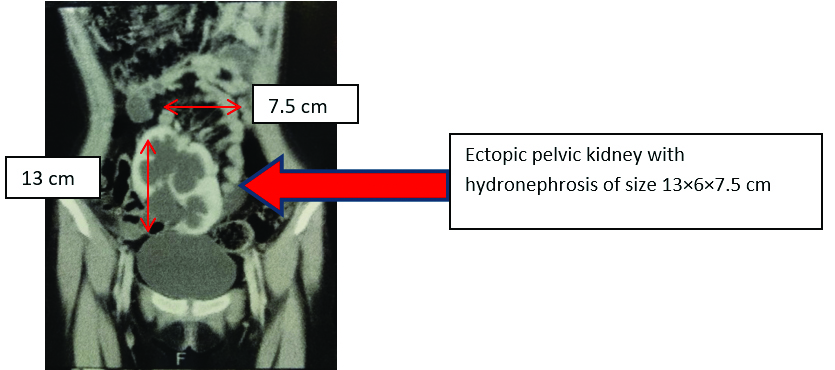
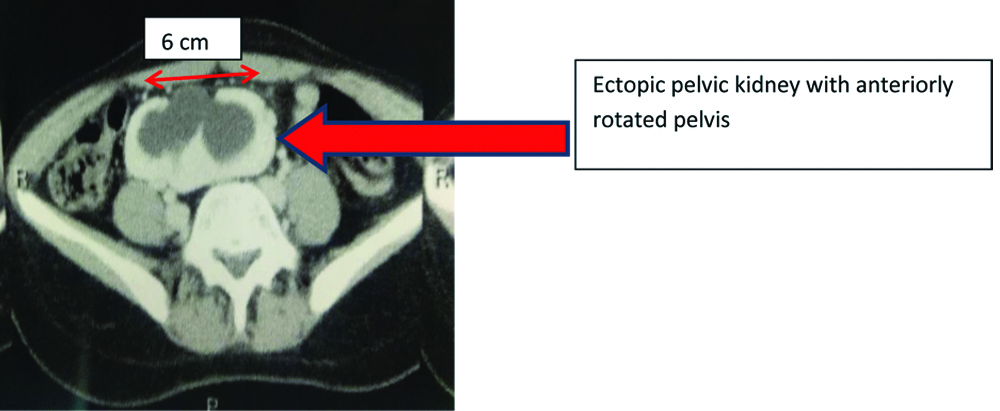
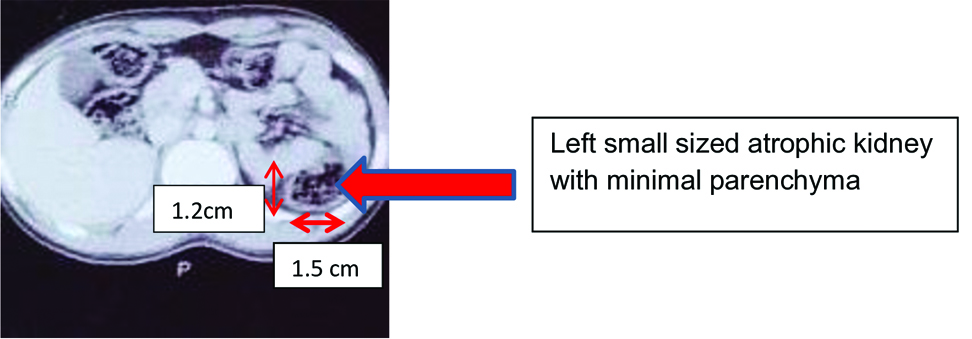
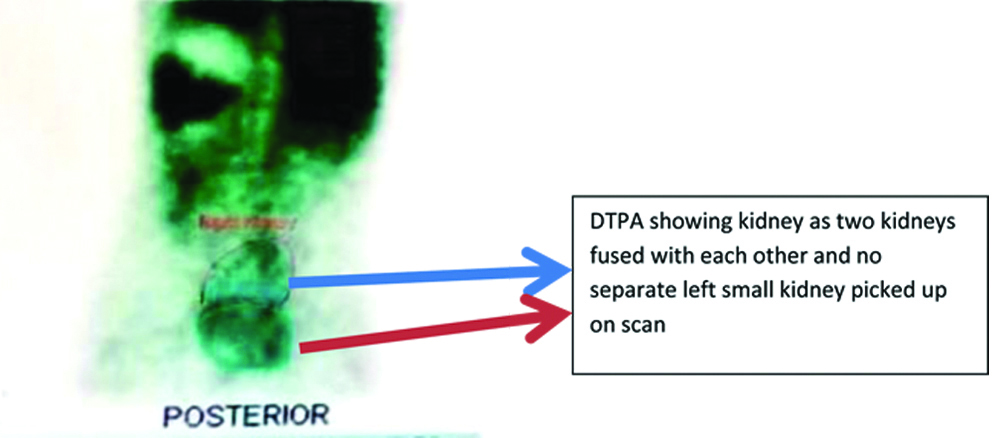
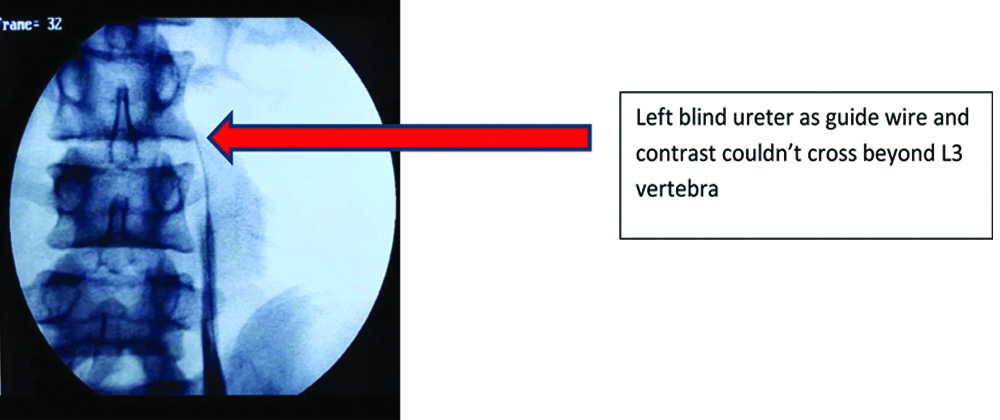
Right pelvis appears bifid in nature. Axial cut of CT IVU which shows that renal pelvis is anteriorly rotated is shown in [Table/Fig-2]. Left small 2.2×1.2×1.5 cm reniform structure noted in left renal fossa suggestive of atrophic left kidney with no parenchymal enhancement in contrast images [Table/Fig-3]. But DTPA mentioned crossed fused kidneys [Table/Fig-4]. So, it was decided to do cystoscopy and retrograde pyelogram. Cystoscopy showed bilateral ureteric orifices at normal positions. Left ureteric catherisation done with 0.035 inch guide wire. Guide wire did not cross to opposite side thus ruling out diagnosis of crossed fused kidney which was seen in DTPA. Guide wire could be passed till L3 vertebra. Left retrograde pyelogram showed blind left ureter till L3 level. As contrast and guide wire were not able to cross ureter beyond L3 vertebral level it seemed blind or atretic ureter [Table/Fig-5].
Left small atrophic kidney with minimal parenchyma.
DTPA showing crossed fused kidneys.
Left blind ureter till L3 vertebra.
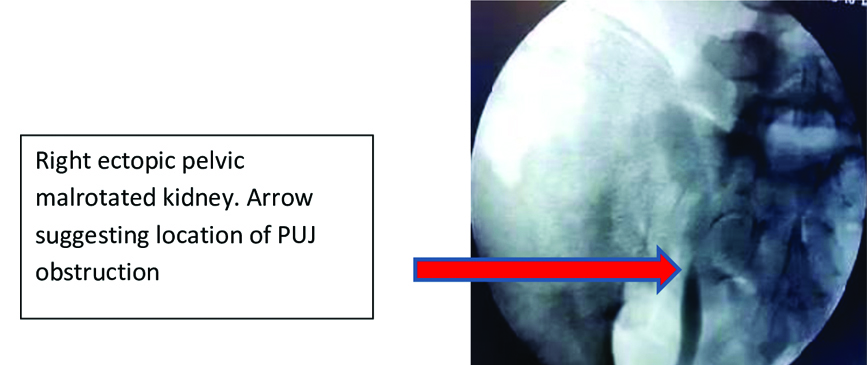
Right-side retrograde pyelogram showed single pelvicalyceal system in pelvic region with abrupt narrowing and delayed drainage suggestive of right PUJO [Table/Fig-6].
Right ectopic pelvic malrotated kidney with arrow pointing to site of PUJO.
So, it was confirmed that two kidneys were not fused. Right one was pelvic region and left kidney was atrophic as seen in CT scan and DTPA report was fallacious. Final diagnosis of right ectopic solitary functioning obstructive kidney due to PUJO was made. And hence surgical option of treatment was offered to patient.
Decision was made to do open pyeloplasty. Pfannenstiel incision with slight curvilinear extension on right-side was taken. Intraoperative findings were:
Malrotated kidney
Anteriorly facing pelvis
Anteriorly faced pelvis with narrowing at PU junction seen. Anderson Hynes pyeloplasty was performed [Table/Fig-7]. Pelvis was opened in diamond shaped fashion. Double J stent was placed. Anastomosis of pelvis and ureter was dependent, wide mouth, tension free and water tight.
Pelvis being sutured to ureter.
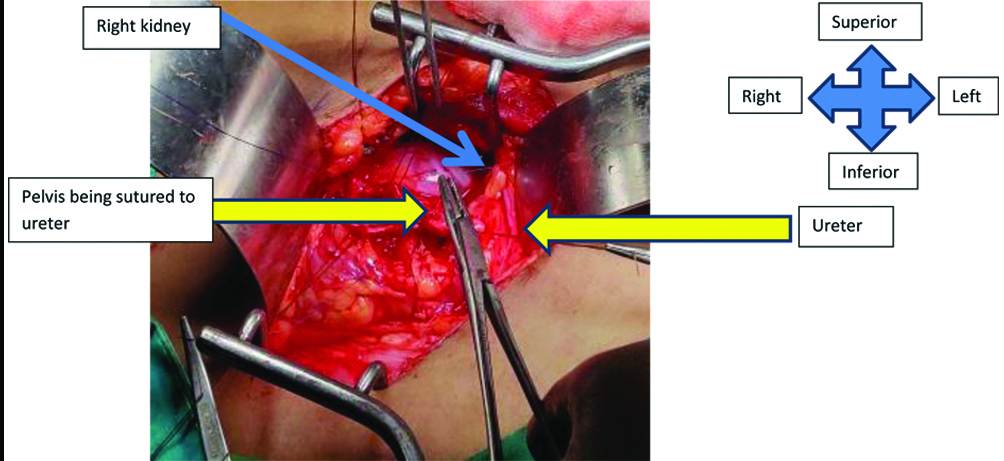
As anomalous kidneys usually have abnormal blood supply it made surgery challenging. Abnormal position of kidney, malrotation made surgery difficult. Foley’s catheter was removed on postoperative day 3. Drain was removed on postoperative day 4. On follow-up sutures were removed on postoperative day 10. After one month follow-up the patient is symptomatically better as patient has no complaint of pain and there is no need for analgesics.
Discussion
The ectopic kidney is generally is seen on left side. Incidence of single solitary ectopic kidney is found as 1 in 22,000 autopsies. PUJO was found in one in seven neonates which were having antenatal hydronephrosis [1-3]. PUJO is one of the common congenital anomaly. Incidence of PUJO is nearly one in 1000 to about one in 2000 live births [2-4]. DTPA is usually used in diagnosis of pelviureteric junction obstruction. Aperistaltic segment at the PUJ is the most common cause of PUJO causing functional obstruction [3]. Location of ectopic kidney differs and it can be lumbar or pelvic. Pelvic kidney has incidence of around 1 in 2,200 and 1 in 3,000 [5]. Renal scintigraphy helps to determine renal anatomy, perfusion and function as well. It is mainly used for perfusion and function. Because majority of the times renal anatomy is evaluated with CT scan, ultrasonography and Magnetic Resonance Imaging (MRI). It can be used on special occasions like contrast material allergy, abnormal renal function and altered Glomerulus Filtration Rate (GFR). It can be used in patients with claustrophobia. The present case presents urological anomaly in which CT reported right kidney is ectopic and situated in pelvic region and left kidney small atrophic in nature. On the contrary DTPA did not detected left kidney in its normal position and mentioned both kidneys fused with each other, left being crossed and fused with right kidney. Also, during cystoscopy and retrograde pyelogram it cleared the diagnostic dilemma as in left retrograde pyelogram didn’t cross midline and diagnosis of left crossed kidney was ruled out. Cases of ectopic kidney and PUJO are described in [Table/Fig-8] [6-9].
Comparison with similar case reports [6-9].
| Authors | Age/Gender | Complaints | Finding | Treatment |
|---|
| Hajji F et al., [6] | 47/F | Right flank pain with abdominal swelling | Right renal PUJO with left crossed fused kidney | DJ (double-J) stenting |
| Kato T et al., [7] | 15/M | Right flank pain | Right obstructed pelvis due to left crossed fused kidney with left PUJO | Right nephrostomy followed by left pyeloplasty |
| Daoud MF et al., [8] | 39/M | Left flank pain | Both ectopic kidneys with left PUJO | Left open pyeloplasty |
| Muruganandham K et al., [9] | 16/F | Abdominal pain | Left crossed fused kidney and left PUJO | Laparoscopic pyeloplasty |
| Current study | 19/F | Pain in abdomen | Right ectopic kidney with PUJO with left small atrophic kidney | Open right pyeloplasty |
Conclusion(s)
In cases of renal anomalous pathologies collective use of proper imaging studies and discussion with respective Departments regarding the same and retrograde pyelogram may help decide and improve treatment and better outcome and avoid diagnosis turmoil as seen in present case.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jun 19, 2024
Manual Googling: Jul 23, 2024
iThenticate Software: Aug 21, 2024 (6%)
[1]. Ismaili K, Avni FE, Wissing KM, Hall M, Brussels Free University Perinatal Nephrology Study GroupLong-term clinical outcome of infants with mild and moderate fetal pyelectasis: Validation of neonatal ultrasound as a screening tool to detect significant nephrouropathiesJ Pediatr 2004 144(6):759-65. [Google Scholar]
[2]. Jaswon MS, Dibble L, Puri S, Davis J, Young J, Dave R, Prospective study of outcome in antenatally diagnosed renal pelvis dilatationArch Dis Child Fetal Neonatal Ed 1999 80(2):F135-38. [Google Scholar]
[3]. Woodward M, Frank D, Postnatal management of antenatal hydronephrosisBJU Int 2002 89(2):149-56. [Google Scholar]
[4]. Morris RK, Kilby MD, Congenital urinary tract obstructionBest Pract Res Clin Obstet Gynaecol 2008 22(1):97-122. [Google Scholar]
[5]. Cinman NM, Okeke Z, Smith AD, Pelvic kidney: Associated diseases and treatmentJ Endourol 2007 21(8):836-42. [Google Scholar]
[6]. Hajji F, Moufid K, Ghoundale O, Touiti D, A rare case of pelviureteric junction obstruction in the uncrossed kidney of a crossed fused renal ectopiaAnn R Coll Surg Engl 2018 100(8):e01-03. [Google Scholar]
[7]. Kato T, Aoki M, Torii K, Hamakawa T, Nishio H, Mizuno K, Pelviureteric junction obstruction of the ipsilateral kidney caused by hydronephrosis secondary to crossed fused renal ectopiaIJU Case Rep 2022 5(5):354-57. [Google Scholar]
[8]. Daoud MF, Chaachou A, Marrak M, Raboudi M, Dridi M, Ghozzi S, Bilateral ectopic pelvic kidney associated to left ureteropelvic junction syndrome: A case reportUrol Case Rep 2022 45:102289 [Google Scholar]
[9]. Muruganandham K, Kumar A, Kumar S, Laparoscopic pyeloplasty for ureteropelvic junction obstruction in crossed fused ectopic pelvic kidneyKorean J Urol 2014 55(11):764-67. [Google Scholar]