Abdominal Epilepsy (AE) is a rare and often under-recognised form of epilepsy that typically presents in children with gastrointestinal symptoms, such as recurrent vomiting. This condition can easily be misdiagnosed due to its atypical presentation, leading to delayed treatment and prolonged distress for patients and their families. Despite its rarity, AE should be considered in children with unexplained recurrent vomiting, particularly when other diagnoses fail to explain the symptoms. This is a unique case report of a 14-year-old boy who presented with a history of headache, persistent vomiting and dehydration that did not resolve with initial conservative treatment. Given the persistent nature of his symptoms, an Electroencephalogram (EEG) was performed, which confirmed the diagnosis of AE. The EEG revealed characteristic epileptic discharges that were not initially recognised as related to gastrointestinal symptoms. Following the diagnosis, the patient was started on sodium valproate, which led to a significant improvement in his symptoms. This case highlights the importance of considering AE in children with recurrent vomiting, especially when initial treatments do not yield results. It underscores the need for careful diagnostic work-up, including EEG and appropriate treatment with anticonvulsants.
Case Report
A 14-year-old boy presented with complaints of a sudden, diffuse headache lasting for one day, with no aggravating or relieving factors. He also experienced six to seven episodes of non projectile, non bilious vomiting. There were no associated symptoms such as photophobia, blurred vision, or other visual disturbances. The patient reported a history of similar headache episodes over the past one month, occurring with a frequency of four times, each episode lasting one or two days. These episodes were associated with redness of the eyes, which relieved with rest. No medical management had been sought for these episodes. Additionally, the patient experienced lethargy and excessive tiredness during these episodes. His oral intake was reduced, and he passed urine only twice on the day of admission. There were no such incidents previously. The patient is developmentally normal for his age and there is a family history of migraine in his father and elder brother.
On examination, vital parameters such as temperature, pulse rate, respiratory rate and blood pressure were found to be normal. The child appeared dull but was conscious and oriented to time, place and person; his eyes were sunken, and his lips were dry. Systemic examination was normal. The child was admitted, and the dehydration was corrected with appropriate intravenous fluids. Treated symptomatically with Inj. Ondansetron (0.15 mg/kg/dose) via the intravenous route and Inj. Paracetamol (10 mg/kg/dose) also via the intravenous route for one day. Vitals and urine output were monitored every second hourly. After initial stabilisation, hydration status improved and urine output became normal.
Based on the clinical history provided, the differential diagnosis included acute gastritis, abdominal migraine, cyclic vomiting syndrome, intracranial space-occupying lesions and AE.
On investigating, the child’s complete blood count, serum electrolytes, capillary blood glucose, urine routine analysis, renal function test, liver function test and ultrasound abdomen were normal. He had persistent headaches and six episodes of vomiting, even after receiving paracetamol and antiemetics. The child was drowsy and lethargic, but his vital parameters were found to be normal. A brain Magnetic Resonance Imaging (MRI) was performed, and the results were normal. The ophthalmological examination also found to be normal.
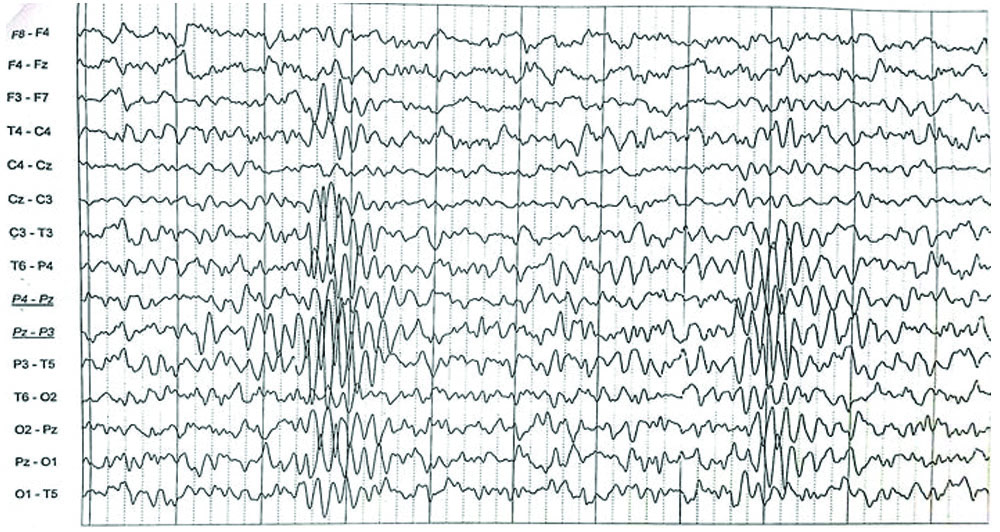
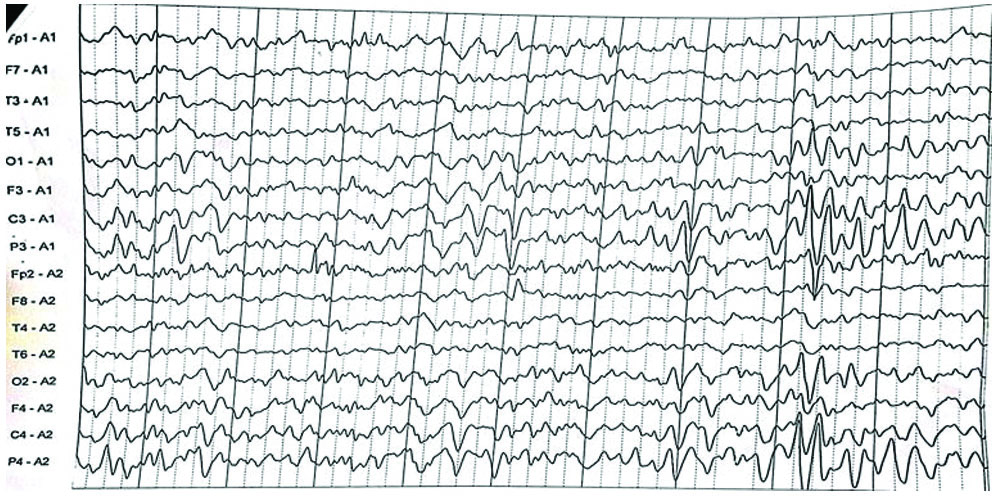
In view of persistent, intense headache, the Magnetic Resonance Angiography-Magnetic Resonance Venography (MRA-MRV) study was done to rule out vascular malformations, venous sinus thrombosis and intracranial hypertension, which all returned normal results. Given the recurrent episodes of cyclical vomiting and the lack of any identifiable organic pathology in the tests, AE was considered a potential diagnosis. To confirm it, an EEG was done, and it exhibited abnormal epileptiform activity with sharp polyphasic waves in the left parietotemporal region [Table/Fig-1a]. The same abnormal epileptiform activity was confirmed when viewed in the average montage [Table/Fig-1b].
Electroencephalogram (EEG) shows sharp polyphasic waves in the left parietotemporal region.
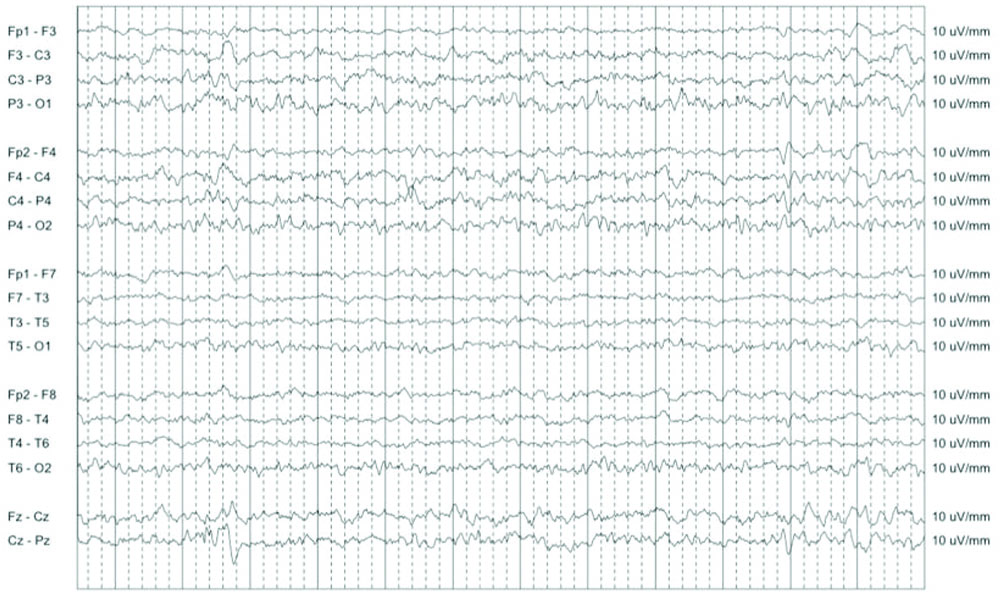
Following the investigations, the child was started on tablet sodium valproate 200 mg once daily, with a plan of duration of two years. Child improved dramatically after the antiepileptic drug. Oral feeds were well tolerated. The child was observed for two days and was symptom-free, and the patient was discharged, with Tablet sodium valproate at a dosage of 20 mg/kg/day. Subsequent follow-up visits every month demonstrated a favourable response to treatment, with the patient remaining asymptomatic until the last follow-up, one year after discharge. After one year of treatment, the child had no episodes of headache or vomiting; weight gain was present and he was advised regarding balanced nutrition and physical activity. Repeat EEG was done after one year showed no epileptiform activity, as shown in [Table/Fig-1c].
Electroencephalogram (EEG) taken after one year of treatment.
Discussion
Epilepsy is a neurological condition marked by recurrent, unprovoked seizures. Although seizures are typically associated with altered consciousness, abnormal movements, or sensory disturbances, there are atypical forms of epilepsy that can present with distinctive symptoms. The AE, a relatively rare form of seizure disorder, occurs primarily in children [1]. AE is a rare disorder most seen in children, involving gastrointestinal disturbances due to epileptic activity. It is described as a type of temporal lobe epilepsy. Response to antiepileptic drugs may aid in diagnosis. The disease was first described by Trousseau in 1868 in a boy with paroxysmal gastrointestinal symptoms leading to grand mal seizures. Moore MT provided the first report of AE supported by electroencephalographic findings in 1944 [2].
Clinical and epidemiological data from the Indian subcontinent, especially in the paediatric subpopulation, are few [3]. The pathophysiology of AE remains unclear. Several possible causes have been considered, such as prematurity, febrile convulsions and neuroendocrine dysfunction, but these have not been conclusive [4]. One hypothesis to explain the mechanism of AE is the presence of abnormal waves in the temporal lobe and amygdala. Through the dorsal motor nucleus of the vagus nerve, the amygdala transmits neurotransmission to the gastrointestinal tract. The amygdala is also thought to play a role in transmitting disease to the hypothalamus, which then activates sympathetic pathways and causes gastrointestinal symptoms [5]. EEGs often show a series of slow high-voltage waves, generalised spikes, saccade discharges, or focal abnormalities, especially in the temporal lobe.
Diagnostic Criteria
AE is characterised by the following diagnostic criteria [5,6]:
Otherwise unexplained, paroxysmal GI symptoms like abdominal pain, nausea, vomiting;
Symptoms of Central Nervous System (CNS) disturbance, such as alterations in mental status, headache, dizziness, or convulsions;
An abnormal EEG with findings specific for seizure disorder;
Improvement with anticonvulsant medication.
In this case report, all the four diagnostic criteria mentioned above were met. However, there are no recommendations regarding the choice of anticonvulsant to use. Several drugs, either alone or in combination, have been used in treatment. Kshirsagar VY et al., and Dutta SR et al., found that oxcarbazepine significantly reduced symptoms in patients [7,8]. Yunus Y et al., reported that treatment with valproic acid in AE, like this case, rapidly improved the patient’s abdominal symptoms [9]. The choice of medication may vary based on the individual patient’s response and tolerability. Patient and family education is crucial to ensure medication compliance and prompt recognition of seizure triggers or warning signs. Regular follow-up with a healthcare provider is necessary to monitor treatment effectiveness and adjust medications as needed [1].
Mondal R et al., from Siliguri, in 2014, compiled a case series of six patients diagnosed with AE, noting that, except for two patients who experienced recurrent vomiting, recurrent abdominal pain was a prevalent occurrence among all the other patients, they were treated with antiepileptic medication and responded well [3]. Dutta SR et al., from Assam, in 2007, published a case series of three cases of AE, one of which affected an adult. All the three patients had abdominal pain as the predominant symptom. They responded well to antiepileptic medication [8]. Singhi PD and Kaur S et al., reported on a 10-year-old boy from Chandigarh who suffered from recurrent paroxysmal abdominal pain. Initially treated as psychogenic pain, the patient was later diagnosed with AE based on EEG findings. The pain responded well to antiepileptic treatment [10].
Most of the case reports available in the literature have documented abdominal pain as the primary symptom; whereas in the present case, persistent vomiting and headache as the predominant symptom. Irrespective of the semiology reported in the various case reports, most of the patients responded well to antiepileptic drugs.
The differential diagnosis suspected in this case are discussed below [Table/Fig-2] [11].
Differential diagnosis for recurrent vomiting, abdominal pain with headache in children [11].
| Abdominal Epilepsy (AE) | Abdominal migraine | Cyclical vomiting
syndrome |
|---|
| Abdominal pain is abrupt in onset with relatively short duration of episode. It can present as other GI symptoms and associated with CNS manifestations like headache. | Abdominal pain episodes separated by weeks or months. At least a 6-month period before diagnosis. Headache is not a prominent feature during attacks. | Episodic attacks of intense nausea and paroxysmal vomiting lasting hours to days within a 6-month period. Vomiting during attacks occurs at least 4 times/hr,12-15 episodes/day. Headache is less prominent feature. |
| Age: 8-12 years. | Age: 2-10 years. | Age: Median age of onset is 5 years. |
| Pain is followed by post ictal sleep or dizziness or lethargy. | No such episode. | Dehydration may be present. |
| Not functional disorder. | A functional disorder diagnosed by ROME III H2c criteria. | Not attributable to another disorder. A functional disorder. |
| EEG changes will be present. | EEG will be normal. | EEG will be normal/abnormal. |
Conclusion(s)
The AE is a rare condition that can cause recurrent vomiting and headaches in children. Gastrointestinal and neurological symptoms should be specifically questioned by the attending physician. An EEG is a crucial diagnostic tool for AE. Treatment with antiepileptic drugs is known to be well tolerated in this setting. AE should be considered as a differential diagnosis in children with recurrent headaches and vomiting, after excluding life-threatening causes, thus avoiding misinterpretation of these symptoms as “functional” or “psychogenic” allowing for early diagnosis and treatment.
[1]. Saad K, Samir A, Abdelall H, Abdel G, Nahed S, Ahmed M, Abdominal epilepsy in children: A comprehensive overviewInt J Med Res 2023 2:36-38. [Google Scholar]
[2]. Duncan DM, Ngosa M, Mwiche S, Womba K, Muhumpu K, Abdominal epilepsy: A case presentationInt J Healthcare Sci 2016 4(1):196 [Google Scholar]
[3]. Mondal R, Sarkar S, Bag T, Mondal K, Saren A, A paediatric case series of abdominal epilepsyWorld J Pediatr 2014 10(1):80-82.10.1007/s12519-014-0457-124464669 [Google Scholar] [CrossRef] [PubMed]
[4]. Franzon RC, Lopes CF, Schmutzler KM, Moreis MI, Guerreiro MM, Recurrent abdominal pain: When an epileptic seizure should be suspected?Arquivos de Neuro-Psiquiatria 2002 60(3-A):628-30.10.1590/S0004-282X200200040002112244404 [Google Scholar] [CrossRef] [PubMed]
[5]. Chamida FM, Khalida NM, Abdominal epilepsy, a diagnosis to consider in children with recurrent vomiting: A case reportAsian J Heal Res 2023 2(1):84-88.10.55561/ajhr.v2i1.76 [Google Scholar] [CrossRef]
[6]. Mpondo BCT, Mwasada G, Nyundo AA, Abdominal epilepsy, an uncommon cause of chronic and recurrent abdominal pain: A case reportClin Case Reports [Internet] 2016 4(12):1117-19.10.1002/ccr3.71127980744PMC5134139 [Google Scholar] [CrossRef] [PubMed]
[7]. Kshirsagar VY, Nagarsenkar S, Ahmed M, Abdominal epilepsy in chronic recurrent abdominal painJ Pediatr Neurosci 2012 7:163-66.10.4103/1817-1745.10646823559997PMC3611899 [Google Scholar] [CrossRef] [PubMed]
[8]. Dutta SR, Hazarika I, Chakravarty BP, Abdominal epilepsy, an uncommon cause of recurrent abdominal pain: A brief reportGut 2007 56:439-41.10.1136/gut.2006.09425017339252PMC1856820 [Google Scholar] [CrossRef] [PubMed]
[9]. Yunus Y, Sefer U, Dondu UU, Abdominal epilepsy as an unusual cause of abdominal pain: A case reportAfr Health Sci 2016 16(3):877-79.10.4314/has.v16i3.3227917225PMC5111992 [Google Scholar] [CrossRef] [PubMed]
[10]. Singhi PD, Kaur S, Abdominal epilepsy misdiagnosed as psychogenic painPostgrad Med J 1988 64(750):281-82.10.1136/pgmj.64.750.2813186570PMC2428499 [Google Scholar] [CrossRef] [PubMed]
[11]. Deswal S, Paul P, Murugan S, Yadav TP, Abdominal epilepsy- A diagnosis often missed! - A case reportPediatric Rev: Int J Pediatrics Res [Internet] 2018 5(11):598-600.10.17511/ijpr.2018.i11.09 [Google Scholar] [CrossRef]