Third molars are present in 90% of the population with 33% having at least one impacted third molar. Thus, surgical removal of impacted third molar is the most frequently performed procedure [1]. Impacted lower third molar extraction produces a series of side effects, which include pain, inflammation, and trismus [2].
Flap design is one important factor which influences the severity of these complications [3]. Flap design is important, not only for allowing optimal visibility and access to the impacted tooth, but also for subsequent healing of the surgically created defect. With so many objectives, the actual design of a flap sometimes becomes a compromise between peri- and post–operative considerations [4].
The aim of this study was to compare two different flap designs in extraction of impacted mandibular third molars, by assessing their post–operative complications. In this study, pain, swelling, mouth opening and pocket depth were selected as parameters for comparing the two flap designs.
Material and Method
This study was a hospital based, experimental study with a “cross–over” design, which was done on thirty patients. Patients with bilateral, completely impacted, mandibular third molars or partially erupted third molars, without any symptoms of pain or swelling, who had good oral hygiene, were included in the study. Patients who were on any medications, lady patients who were pregnant, patients with severe pericoronitis, patients with soft tissue impaction and patients who were medically compromised were excluded from study.
Thirty patients who satisfied the inclusion criteria were enrolled in the study after getting their consents. Assessment of the position, class and depth of the impacted teeth was done by using OPG. Pre–operative measurements of pain, swelling, mouth opening and pocket depth were recorded. Surgical removal of one side impacted mandibular third molar was done under local anaesthesia. Standard flap incisions were made on one side of the lower jaw in randomly chosen patients.
Post–operative measurements of pain, swelling and mouth opening were measured on days 1, 3 and 7 respectively. A wash out period of at least 10 days after the 7th day of surgery was given and the patient was recalled on the 25th day. The extraction of the impacted teeth on the opposite side of the lower jaw was done, with the alternate flap design—a comma incision. The follow up and post–operative complications of patients on days 1, 3 and 7 were recorded for the parameters which were studied. The pocket depth was measured for both sides at the end of first month and the second month. The criteria which were standardized by Dr. Nageshwar (Nageshwar 2002) were followed for measuring these parameters.
Flap Designs:
Standard Incision:
Ward’s Incision [Table/Fig-1]:
Standard Incision Ward’s Incision
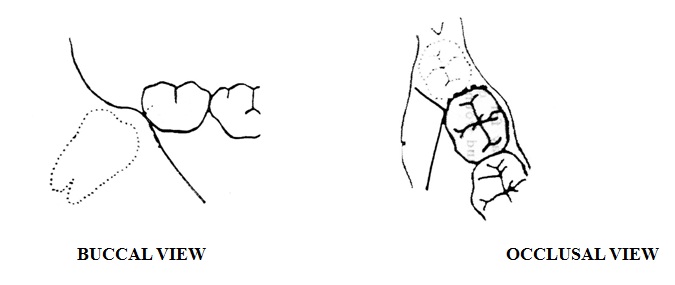
Anterior incision curves forward from the distobuccal corner of the crown of the lower second molar and it ends alongside the mesiobuccal cusp of that tooth. Incision is then extended distally level with the buccal side of the tooth to the external oblique ridge. If the anterior part of the flap is elevated from the bone, one blade of a pair of scissors may be inserted onto the surfaces of the bone and the incision may be completed by closing the blades. Posterior part of the incision must slope outwards as well as backwards, as the ascending ramus lies on the lateral side of the body of the mandible.
Modified Ward’s Incision [Table/Fig-2]:
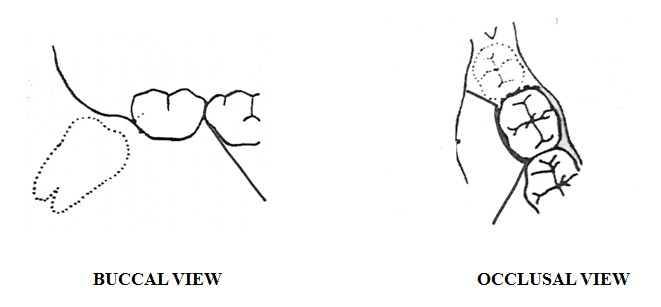
Anterior incision curves forward from the distobuccal corner of the crown of the lower first molar and it ends alongside the mesiobuccal cusp of that tooth. A vertical or crevicular incision should be made through the buccal gingival crevice of the second molar. Incision is then extended distally level with the buccal side of the tooth to the external oblique ridge. If the anterior part of the flap is elevated from the bone, one blade of a pair of scissors may be inserted onto the surfaces of the bone and the incision may be completed by closing the blades. Posterior part of the incision must slope outwards as well as backwards, as the ascending ramus lies on the lateral side of the body of the mandible [Table/Fig-3].
Surgical Removal of 38 Using Standard Ward’s Incision
Comma Incision [Table/Fig-4]
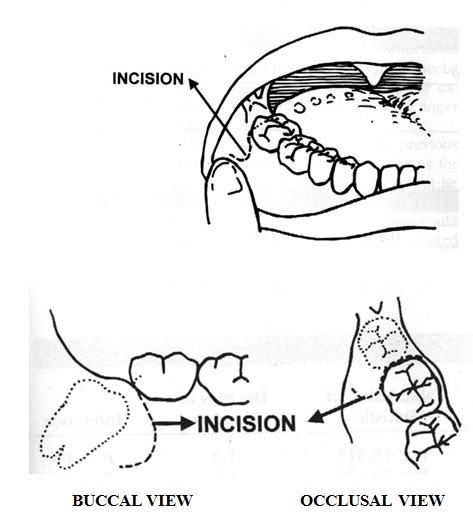
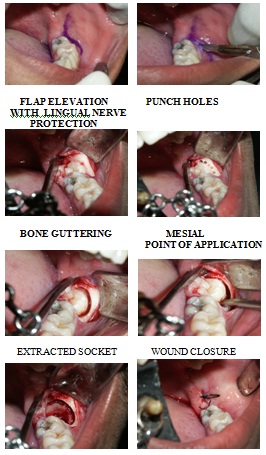
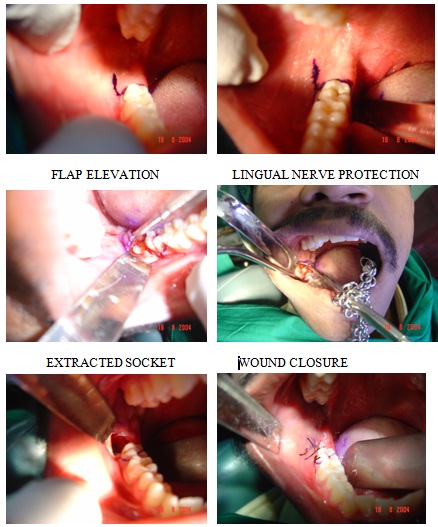
Starting from a point which is at the depth of stretched vestibular reflection which is posterior to the distal aspect of the preceding second molar, the incision is made in an anterior direction. Incision is made to a point below the second molar, from where it is smoothly curved up to meet the gingival crest at the distobuccal line angle of the second molar. The incision is continued as a crevicular incision around the distal aspect of the second molar (a distolingually based flap) [Table/Fig-5]. After reflection of the flap, common steps for removal of impacted third mandibular molars are followed, that is retraction of the buccal mucosa (Austin’s retractor) and lingual mucosa. Thelingual nerve is protected along with the linguo mucoperiosteum by Rugieme end of Howarths elevator and it is held by chain of Meckessons mouth prop. After exposing the bone around the tooth by using a straight shank surgical 703 bur, punch holes are made around the tooth and bone is guttered by the bur, with adequate saline irrigation.
Surgical Removal of 48 Using Comma Incision
Data Management and Analysis
The sample size in this study was 27 and after considering drop outs, 30 patients with bilateral impaction were included in the study, but ten patients were lost to follow up after they underwent extractions on one side. Statistical analyses were done by using the data which was collected from twenty patients only. Wilcoxon Signed Ranks was used to compare the post–operative complications, pain, swelling and mouth opening between the standard and comma incisions.
Paired ‘t’–test was used to compare the mean pockets depth between the standard and comma incisions.
Kruskal–Wallis test was used to analyze the post–operative complications in standard and comma incisions over time.
Results
In extractions which were done by making standard incisions, 45% of subjects were found to have severe pain on day 1, whereas only 15% of subjects had severe pain in the extractions which were done by using comma incisions. It was found that there was a highly statistically significant difference between the two types of incisions on day 1 on comparing the pain. (Z=-3.46, p = .001). Similarly, the pain was severe for 5% of the patients who had undergone extractions with standard incisions and there was no patient with severe pain on the 7th day in whom extractions were done by making comma incisions.(Z =-3.45, p=.001) [Table/Fig- 6].
Subjective assessment of pain in relation to standard and comma incision
| Factors | Standard Incision | Comma Incision | Z | p value |
|---|
| Pain | No. | % | No. | % |
|---|
| Preoperative | | | | | | |
| Absent | 20 | 100 | 20 | 100 | | |
| Mild | 0 | 0 | 0 | 0 | .000 | 1.00 |
| Moderate | 0 | 0 | 0 | 0 | | |
| Severe | 0 | 0 | 0 | 0 | | |
| Day 1 | | | | | | |
| Absent | 0 | 0 | 0 | 0 | | |
| Mild | 1 | 5 | 7 | 35 | - 3.46 | .001 |
| Moderate | 10 | 50 | 10 | 50 | | |
| Severe | 9 | 45 | 3 | 15 | | |
| Day 3 | | | | | | |
| Absent | 0 | 0 | 0 | 0 | | |
| Mild | 7 | 35 | 3 | 25 | - 3.09 | .002 |
| Moderate | 8 | 35 | 11 | 50 | | |
| Severe | 5 | 30 | 6 | 25 | | |
| Day 7 | | | | | | |
| Absent | 3 | 15 | 12 | 60 | | |
| Mild | 9 | 45 | 8 | 40 | - 3.45 | .001 |
| Moderate | 7 | 35 | 0 | 0 | | |
| Severe | 1 | 5 | 0 | 0 | | |
It was found that there was no statistically significant difference between the two types of incisions on day 1 on comparing the swelling. (Z=-.632, p=.527). The swelling was severe for 20% of the patients who had undergone extractions with standard incisions and it was only 5% in patients on the 3rd day in whom extractions were done by using comma incisions. (Z =-2.24, p=.025). There was a statistical difference between both groups on day 7 also (Z=-1.99, p = .046) [Table/Fig-7].
Comparison of standard incision with comma incision in relation to swelling
| Factors | Standard Incision | Comma Incision | Z | p value |
|---|
| Pain | No. | % | No. | % |
|---|
| Preoperative | | | | | | |
| Absent | 20 | 100 | 20 | 100 | | |
| Mild | 0 | 0 | 0 | 0 | .000 | 1.00 |
| Moderate | 0 | 0 | 0 | 0 | | |
| Severe | 0 | 0 | 0 | 0 | | |
| Day 1 | | | | | | |
| Absent | 0 | 0 | 0 | 0 | | |
| Mild | 3 | 15 | 1 | 5 | - .632 | .527 |
| Moderate | 8 | 40 | 14 | 70 | | |
| Severe | 9 | 45 | 5 | 25 | | |
| Day 3 | | | | | | |
| Absent | 0 | 0 | 2 | 10 | | |
| Mild | 8 | 40 | 11 | 55 | - 2.24 | .025 |
| Moderate | 8 | 40 | 16 | 30 | | |
| Severe | 4 | 20 | 1 | 5 | | |
| Day 7 | | | | | | |
| Absent | 7 | 35 | 12 | 60 | | |
| Mild | 9 | 45 | 7 | 35 | - 1.99 | .046 |
| Moderate | 4 | 20 | 1 | 5 | | |
| Severe | 0 | 0 | 0 | 0 | | |
The mouth opening on day 1 on standard incision side of between 29 – 25 mm was 35%, whereas only 10% of the patients interincisal distance measurement lied between this value in comma incision side. It was found that there was a highly statistically significant difference between the two incisions on comparing the mouth opening on day 1(Z = - 3.87, p value = 0.00). But though there was a clinical difference between the two incisions on days 3 and 7, there was no statistical significance [Table/Fig- 8].
Comparison of the two incisions with respect to mouth opening
| Factors | Standard Incision | Comma Incision | Z | p value |
|---|
| Mouth Opening | No. | % | No. | % |
|---|
| Preoperative | | | | | | |
| 55 – 50 | 5 | 25 | 5 | 25 | | |
| 49 – 45 | 9 | 45 | 9 | 45 | | |
| 44 – 40 | 6 | 30 | 6 | 30 | .000 | 1.00 |
| 39 – 35 | 0 | 0 | 0 | 0 | | |
| 34 – 30 | 0 | 0 | 0 | 0 | | |
| 29 – 25 | 0 | 0 | 0 | 0 | | |
| Day 1 | | | | | | |
| 55 – 50 | 0 | 0 | 0 | 0 | | |
| 49 – 45 | 0 | 0 | 0 | 0 | | |
| 44 – 40 | 0 | 0 | 2 | 10 | - 3.87 | .000 |
| 39 – 35 | 4 | 20 | 10 | 50 | | |
| 34 – 30 | 9 | 45 | 6 | 30 | | |
| 29 – 25 | 7 | 35 | 2 | 10 | | |
| Day 3 | | | | | | |
| 55 – 50 | 0 | 0 | 0 | 0 | | |
| 49 – 45 | 3 | 15 | 5 | 25 | | |
| 44 – 40 | 8 | 40 | 9 | 45 | - 1.67 | .096 |
| 39 – 35 | 9 | 45 | 6 | 30 | | |
| 34 – 30 | 0 | 0 | 0 | 0 | | |
| 29 – 25 | 0 | 0 | 0 | 0 | | |
| Day 7 | | | | | | |
| 55 – 50 | 0 | 0 | 3 | 15 | | |
| 49 – 45 | 10 | 50 | 9 | 45 | | |
| 44 – 40 | 8 | 40 | 8 | 40 | - 1.94 | .052 |
| 39 – 35 | 2 | 10 | 0 | 0 | | |
| 34 – 30 | 0 | 0 | 0 | 0 | | |
| 29 – 25 | 0 | 0 | 0 | 0 | | |
There was no statistical difference between standard incisions and comma incisions in relation to pocket depth which was measured at the end of first month and the second month. However, on comparing standard incisions and comma incisions separately over time, it was found that there was a statistical significance between the pocket depth in first month and the second month (Standard incision – t = 12.78, p value = 0.001, comma incision – t =11.54, p value = 0.001) [Table/Fig- 9].
Comparison of the two incisions with respect to pocket depth on first month and second month
| Incisions | Pocket Depth | t | p value |
|---|
| 1st Month | 2nd Month |
|---|
| Mean | SD | Mean | SD |
|---|
| Standard | 4.90 | 0.68 | 2.98 | 0.66 | 12.78 | 0.001 |
| Comma | 4.90 | 0.81 | 3.00 | 0.61 | 11.54 | 0.001 |
| t value | 0.00 | 0.129 | | |
| p value | 1.00 | 0.899 | | |
Discussion
The incisions which are used to expose impacted third molars can be broadly classified into triangular and envelope types. Regardless of variations in the anterior end of the incisions, all incisions extend posteriorly from the distal aspect of the preceding second molar, towards the ascending ramus. The standard incisions have been modified by several surgeons. The comma shaped incision was designed by Nageshwar and it proved to be superior to the standard incision.
Post–operative pain after third molar surgery presents itself as a localized inflammation with pain of varying intensities. The removal of the impacted third molar and the resultant tissue and cellular destruction cause the release and production of several biochemical mediators which are involved in pain process, particularly, histamine, bradykinin and the prostaglandins [5]. Moderate to severe pain usually develops during the first 12 hours, with the peak intensity showing after about 6 hours when a conventional local anaesthetic is used. The pain then gradually disappears within a few days if the wound heals normally [6].
Lower pain scores were recorded with comma incision sides as compared to standard incision sides, which was similar to that which was seen in the study of Nageshwar [7]. This result did not correlate with the result of Gool et al., as they had elicited that severity in pain after removal of third molars did not appear to be related to the type of incision [8].
The two main contributing factors in the formation of post–operative swelling are trauma and infection. The damage to the soft and hard tissues, which is associated with oral surgical procedures, is the usual cause of the early post–operative swelling. It is most marked after 19–24 hours and it then diminishes after about seven days [9]. The factors which affect the occurrence of pain and swelling include the skill of the surgeon, the extent of the surgical trauma, suturing, age, sex, medication, time of the day and the local flap design [10–12]. Swelling in the area with comma incision was less as compared to the swelling in the area in which the standard incision was done. These results complimented the results of Nageshwar [7].
The comma shaped incision was found to be encountered by less number of subjects with limited mouth opening as compared to the standard incision side, which was in agreement with the Nageshwar’s results. The interrelationship between trismus and pain has been reported in many studies. This hypothesis was confirmed by an electromyographic study, where it was concluded that restricted mouth opening was a voluntary action for avoiding pain [13].
There was a statistical difference in the post–operative probing depth between the first and second months, which was in agreement with the findings of Stephens et al., However, there was no statistically significant difference between the two types of flaps. These results were in agreement with those of many studies which had compared two flap design for the third molar extractions, which were done by Rosa et al., Quee et al., and Schofield et al., who also reported no differences in pocket depth which was related to flap designs [14]. Several literatures have shown an enhanced regrowth of the alveolar bone crest in young patients whose extracted third molars were in their developmental stages. Kugelberg et al., found that deeper periodontal pocket depth after third molar surgery was 3 times more frequent in people who were older than 25 years of age. They showed that the process of periodontal healing after the surgery was correlated with age [15–18].
The extractions were made bilaterally on the same patients and the two techniques were compared intra–individually. Patients who are in need of prophylactic removals of identical bilateral impacted molar teeth represent a unique material, since essentially the same operation can be performed twice on healthy, asymptomatic individuals, who therefore can serve as their own controls in crossover trials. Variations which are caused by individual differences or fluctuations in disease activity can thus be eliminated or minimized. The results which were obtained were statistically significant and it was considered that sufficient information was obtained from the study. This cross–over design greatly enhanced the statistical power and validity of the study.
Conclusion
The results of this study showed that the new incision design was preferable over the conventional method, considering the lesser degree of post–operative complications.