Yolk Sac Tumour of the Cryptorchid Testis, with an Unusual Presentation — Diagnosed by Fine Needle Aspiration Cytology
Dilip Chandra Barman1, Aniket Halder2, Sumanta Bhattacharya3, Krishnendu Mandal4, Sanjay Kumar Mallick5
1 Assistant Professor, Department of Pathology, North Bengal Medical College, Darjeeling, West Bengal, India.
2 Post Graduate Trainee, Department of Pathology, North Bengal Medical College, Darjeeling, West Bengal, India.
3 Post Graduate Trainee, Department of Pathology, North Bengal Medical College, Darjeeling, West Bengal, India.
4 Post Graduate Trainee, Department of Pathology, North Bengal Medical College, Darjeeling, West Bengal, India.
5 Assistant Professor, Department of Microbiology, North Bengal Medical College, Darjeeling, West Bengal, India.
Name, Address, E-Mail Id of The Corresponding Author: Dr Dilip Chandra Barman, Assistant Professor, Department of Pathology, North Bengal Medical College, Darjeeling, West Bengal – 734012, India.
Phone: +91-94743 27035
E-mail: dilip77d@gmail.com
Yolk sac tumour is the most common germ cell tumour in infants and children, with a majority of them arising in the gonads. Rare cases of extra – gonadal germ cell tumours have been described in the literature. We are presenting here, a case of a yolk sac tumour of the cryptorchid testis in a 2 year old child, who initially presented with a mass in the left lobe of the liver, with huge ascites and which posed diagnostic difficulties. The mass was diagnosed as hepatoblastoma on Computed Tomography (CT). Subsequently, CT guided Fine Needle Aspiration Cytology (FNAC) of the liver mass showed the features of a yolk sac tumour. The raised serum Alfa Foetoprotein (AFP) levels corroborated with the cytological diagnosis.
Alfa foetoprotein, Fine needle aspiration cytology, Cryptorchidism, Yolk sac tumour
Case Report
A 2 years old male patient presented with a 5cm x 4cm mass in the right hypochondrium, which gradually increased in size, along with huge ascites since the past 1 month. The initial investigations included a Complete Haemogram (CH), a Chest X – ray and CT scan of the chest and abdomen. The CH, X – ray and CT scan of the chest were within normal limits. The CT scan of the upper abdomen showed a fairly enlarged, 48mm x 39mm, well demarcated, mixed density, space occupying lesion (SOL) in the left lobe of the liver, which did not have any calcification [Table/Fig-1]. Clinico – radiologically, the possibility of a Hepatoblastoma was considered. Hence, an FNA from the liver SOL and estimation of the serum AFP level were suggested.
Axial C.T. image of upper abdomen with oral contrast showing a space occupying lesion in the left lobe of liver

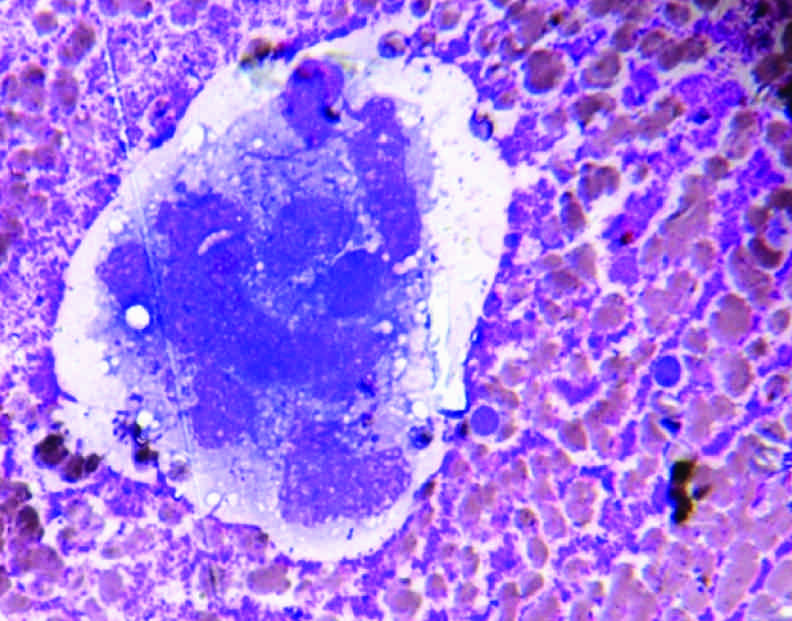
The serum AFP level was found to be markedly raised (1000 ng/ml). So the diagnosis of a hepatoblastoma was made. Thereafter, an FNAC of the liver mass was performed. Alcohol-fixed Haematoxylin and Eosin (H/E) stained smears and air-dried May – Grunwald Giemsa (MGG) stained smears were prepared. The microscopical examination of the smears showed a cellular aspirate of atypical cells which were arranged in papillary fragments, loose clusters and tumour balls, resembled glomeruloid bodies, these cells have large nuclei with opened up chromatin, prominent nucleoli and vacuolated fragile cytoplasm, in a background of mucoid material. Some intracytoplasmic eosinophilic globules were also noted [Table/Fig-2, 3]. Cytopathologically, a diagnosis of an extra gonadal germ cell tumour (GCT) was made, with the possibility of a primary yolk sac tumour of the liver, which corroborated with the markedly raised serum AFP levels (1000 ng/ml). However, this diagnosis became an issue of conflict between us and the clinician, since both the yolk sac tumours and hepatoblastomas are associated with markedly raised serum AFP levels [1].
Microphotograph showing tumour cells with vacuolated cytoplasm [MGG Stain X 100]
Microphotograph showing tumour cells in loose cluster with open chromatin, prominent nucleoli and finely vacuolated cytoplasm [H/E Stain X 100]

The case was followed up and reviewed. Interestingly, around two weeks after the cytological diagnosis was made, a swelling appeared in the left inguinal region, which increased rapidly in size [Table/Fig-4]. An Ultrasonography (USG) of the lower abdomen was done, diagnosed it to be the left sided undescended testis, with hyperechogenicity. The right testis was present in the scrotal sac with a normal echo-texture. USG – guided FNAC of the the left-sided undescended testis was performed, which showed cytological features exactly similar to those observed in the smears made from the liver mass. Hence, the case was diagnosed as a primary yolk sac tumour of the left sided undescended testis, with metastasis to the left lobe of the liver. Thereafter, an orchidectomy was done for histopathological examination, which showed tumour cells arranged in reticulo – cystic and alveolo-glandular patterns, with the presence of a fair number of Schiller – Duval bodies [Table/Fig-5]. The histopathological examination thus confirmed the diagnosis.
Left inguinal swelling proved to be undescended testis on USG

Section showing tumour cells arranged in reticular and microcystic pattern with Schiller Duval bodies [H/E Stain X 100]

Discussion
Yolk sac tumours are malignant germ cell tumours characterized by numerous growth patterns which recapitulate the yolk sac, the allantois and the extra-embryonic mesenchyme. In children, it is the most commonly occurring testicular neoplasm and it is seen in all races, but it is less common in the Blacks, the Native Americans and the Indians [2–4]. The median age at presentation is 16 – 17 months, which may extend for up to 11 years. There is a right sided preponderance. In about 90% of the cases, the patients present with an asymptomatic scrotal mass and 7% present with a history of trauma or an acute onset of pain [2]. About 10 – 20% of the cases have metastasis at presentation [3, 5]. In children, there is a predilection for a haematogenous spread and in 20 – 26% of the cases, the first clinical site of involvement is the lungs [3,6]. In the present case, the initial manifestation was a distant metastasis to the liver.
Hepatoblastoma remains the most common primary hepatic malignancy in children, which comprises approximately 1% of all the paediatric malignancies and it usually occurs in patients who are less than 3 years of age [7]. The serum AFP levels are elevated in 84 – 91% of the cases, with very high titres [1]. Our case presented with a single well demarcated mass in the left lobe of the liver, with a marked elevation of the serum AFP levels (1000 ng/ml). Thus, a clinico-radiological diagnosis of a hepatoblastoma was made.
The CT guided FNA smears from the liver mass showed cytological features suggestive of a yolk sac tumour. So, the possibility of a hepatoblastoma was ruled out and a diagnosis of a primary yolk sac tumour of the liver was made. A primary yolk sac tumour of the liver is a very rare entity [8].
The diagnosis of an extra – gonadal germ cell tumour is made only when there is no evidence of a primary tumour in the testis or the ovary [9]. Since extra-gonadal GCTs are very rare, therefore a thorough clinical examination should be done, to rule out a possible gonadal origin. Over the years, various case series on extra – gonadal GCTs have been reported, which have questioned its true nature. In a majority of them, a primary source was found in the testis or the ovary, which represented a metastatic gonadal tumour [10]. Our case was categorised as having stage III disease and thus was put on a Cisplatin based combination chemotherapy. At present, the child is being followed up, to assess the response to the therapy.
To conclude, we think that this is an unusual presentation of the primary yolk sac tumour of a cryptorchis testis, which first presented with metastasis in the left lobe of the liver. This was clinico-radiologically misdiagnosed as a hepatoblastoma. A precise diagnosis was made by FNAC and it was confirmed by doing a biopsy, which corroborated with the raised AFP levels. So, the patients with such presentations should always be assessed meticulously by doing clinical and radiological examinations, to rule out a primary gonadal origin. FNAC, along with the estimation of the serum AFP levels, forms a very useful tool for diagnosing such tumours and for predicting the therapy.
[1]. Douglass EC, Hepatic malignancies in childhood and adolescence (hepatoblastoma, hepatocellular carcinoma and embryonal sarcoma)Cancer Treat Res 1997 92:201-12. [Google Scholar]
[2]. Kumar V, Abbas KA, Fausto N, Aster JC, Robbins and CotranPathologic basis of disease 2010 8th edPhiladelphiaElsevier:989-90. [Google Scholar]
[3]. Kaplan GW, Cromie WC, Kelalis PP, Silber I, Tank ESJ r, Prepubertal yolk sac testicular tumours—report of the testicular tumour registryJ Urol 1988 140:1109-12. [Google Scholar]
[4]. Li FP, Fraumeni JF, Testicular cancers in children: epidemiologic characteristicsJ Natl Cancer Inst 1972 48:1575-81. [Google Scholar]
[5]. Pinkerton CR, Malignant germ cell tumours in childhoodEur J Cancer 1997 33:895-901. [Google Scholar]
[6]. Brosman SA, Testicular tumours in prepubertal childrenUrology 1979 13:581-8. [Google Scholar]
[7]. Schnater JM, Kohler SE, Lamers WH, Where do we stand with Hepatoblastoma?Cancer 2003 98:668-78. [Google Scholar]
[8]. Wakely PEJ, Krummel TM, Johnson DE, Yolk sac tumour of the liverMod Pathol 1991 4:121-5. [Google Scholar]
[9]. Droz JP, Horwich A, Extra-gonadal germ cell tumoursIn: Comprehensive Textbook of Genitourinary Oncology 2000 2ndNew YorkLippincott Williams and WillkinsVogelzang NJ, Scardino PT, Shipley WU, Doffey DS (Eds) [Google Scholar]
[10]. Johann FK, Praveen S, Christopher CKH, Goh EH, Razman J, Extra-gonadal Germ Cell Tumour – What About the Testis!J Surg Acad 2011 1(1):34-36. [Google Scholar]