Influenza spreads through droplets from infected individuals while speaking, coughing or sneezing. Non human influenza spreads from respiratory or gastrointestinal tracts of infected hosts. Flu can occur throughout the year, but peak occurrence is in the winter months [1,2]. Flu epidemics occur every 6 to 10 years, usually due to antigenic shifts which expose the population to strains to which it has not been exposed previously [3,4]. Pandemic of H1N1 influenza began in Mexico in March 2009 [1]. Swine influenza (H1N1) is a novel influenza A virus which comprises of a re assortment of 4 distinct genetic elements, namely, swine, human, avian, and Eurasian, which combine into a single influenza virus, swine influenza (H1N1). WHO raised worldwide pandemic alert for swine flu on June 11, 2009, which was first of its kind in past 70 years [5]. In India, index cases were reported from Pune [3]. But soon, the epidemic spread to other parts of the country. Present study was conducted to observe clinical profile of admitted patients with confirmed H1N1 swine flu infection and risk factors associated with need of mechanical ventilation and/or death.
Material and Methods
This was an observational prospective study conducted in a tertiary care teaching hospital during August 2009 to December 2011.
Various definitions
Influenza-like illness (ILI): Fever (temperature of 100°F [37.8°C] or greater) with cough or sore throat in the absence of a known cause other than influenza [1–3].
A confirmed case of H1N1 influenza A (swine flu): An individual with an influenza-like illness with a laboratory-confirmed H1N1 influenza A virus detected by RT-PCR or culture [1–3].
Lymphopaenia: Lymphopaenia was defined when lymphocytes were <10%.
Clinical specimens, microbiological investigation for diagnosis of H1N1 swine flu virus
Patients presented to our hospital with Influenza like illness (ILI) were subjected to throat swab testing. Throat swabs were sent for reverse transcriptase polymerase chain reaction to Virology Institute, Alapuzzha, Kerala. Tests were done as per Indian guidelines for swine flu H1N1 infection [2].
Inclusion criteria: All confirmed cases of H1N1 swine flu infection warranting admission were studied.
Exclusion criteria: Patients with negative RT-PCR.
Data collection and assessment
Standardised questionnaire was prepared to collect following details: age, gender, time distribution, co existing medical conditions like diabetes, chronic liver or kidney disease, malignancy, neurological problems like stroke or seizure disorder, presenting symptoms, duration of symptoms, location of admission (isolation ward/intensive care unit (ICU)) and laboratory investigations like complete blood counts, liver function test and renal function test. All confirmed cases of H1N1 infection were treated with Oseltamavir 75 mg twice daily for 5-10 days as per CDC guidelines [6]. The outcomes of interest were need of mechanical ventilation and/or death during hospitalization. Institute’s research committee approved the study, as it was in the interest of public health to collect data on an emerging pathogen like influenza H1N1 A, as issued in guidelines by Ministry of health of India [2].
Statistical Analysis
SPSS software, version 11 was used for statistical analysis. P value was calculated by Chi–square test, p<0.05 was taken as statistically significant. Multivariate analysis was done with binary logistic regression method.
Results
Baseline characteristics
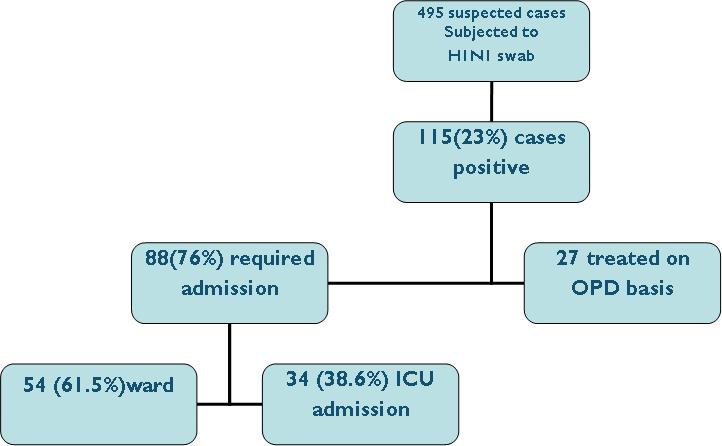
Total 495 patients were presented to our hospital with ILI during the study period and were tested for H1N1 throat swab with RT-PCR. Among them, 115 patients were confirmed to have H1N1 infection. Out of 115 patients, 88 patients required admissions and were included in the study [Table/Fig-1]. Median age of the study cohort was 29 years, with a range of 1-78 years. Baseline demographics of the patient are shown in [Table/Fig-2]. Seventy four percentage of patients belonged to age group of 18-50 [Table/Fig-3].
Outline of study patients
| Variable | n, (%) |
|---|
| Age Mean(SD): 31.6(15.9) | |
| <18 | 11(12.5) |
| 18-50 | 65(73.9) |
| 51-80 | 12(13.6) |
| Gender: Male | 44 (50) |
| Female | 44 (50) |
| Location of admission: | |
| Isolation ward | 54(61.5) |
| ICU isolation | 34(38.6) |
| Presenting symptoms | |
| Fever | 86(97.7) |
| Cough | 76(86.4) |
| Sore thorat | 48(54.5) |
| Dyspnea | 40(45.45) |
| Myalgia | 22(25) |
| Others | 9(10.2) |
| Pneumonia at time of presentation | 58(60.9) |
| Co-morbidity | |
| DM | 12(13.6) |
| CRF | 3(3.4) |
| CLD | 2(2.3) |
| COPD/Asthma | 4(4.5) |
| Pregnancy | 6(6.8) |
| Others(CAD/CNS/Malignancy/OHS) | 15(17)(7/4/2/1/1) |
| Chest X-ray findings | |
| Normal CXR | 37(42) |
| Unilateral consolidation | 9(10.2) |
| Bilateral pneumonia | 38(43.2) |
| Bilateral hilar enlargement | 4(4.5) |
| Outcome | |
| Requirement of Mechanical Ventilation | 14(15.9) |
| Death | 6(6.8) |
*CAD: Coronary artery disease, CNS central nervous system involvement in view of seizure/stroke, OHS: ovarian hyper stimulation syndrome)
Graph showing Age wise Distribution of H1N1 Cases

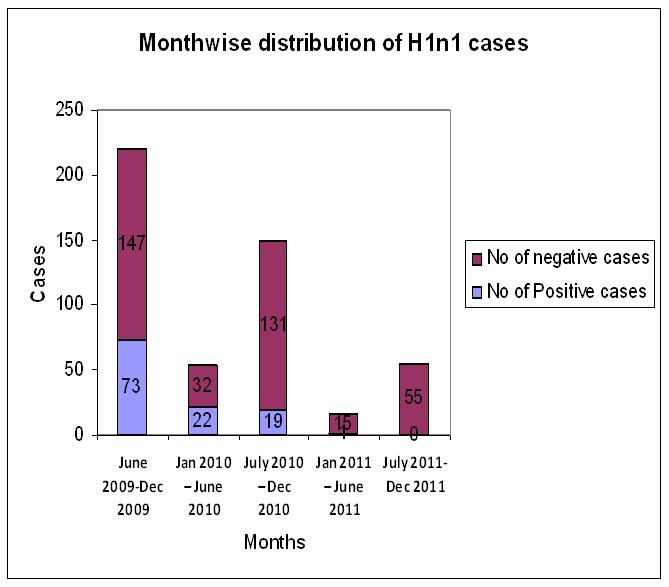
Monthly distribution of H1N1 swine flu cases
Highest occurrence of H1N1 swine flu was observed in August 2009 to June 2010. Overall positivity was 23% (115/495) [Table/Fig-4].
Monthly distribution of H1N1 cases
Clinical symptoms and pre- existing illness at time of presentation
Most common clinical symptom at time of presentation was fever (98%), followed by cough (86%) and sore throat (54%) [Table/Fig-5]. Diabetes mellitus was the most common co-existing medical condition, followed by chronic renal failure, stroke, seizure, malignancy and pregnancy [Table/Fig-2].
Graph showing percentage of clinical symptoms at time of presentation

Isolation of other organisms from sputum in cases of H1N1 infection
All the patients admitted with H1N1 swine flu infection, who had cough with sputum production, were also checked with sputum gram smear and culture to find out co-existing/super added bacterial infection. Out of 88 patients, 73 patients were checked for sputum gram stain and culture. From 73 sputum culture, 20 turned out to be positive for bacteria. Extended spectrum betalactamase producing Klebsiella and non fermenting gram negative bacilli Acinetobacter baumanni were seen in 6 cases each, followed by Streptococcus pneumoniae in 4 cases and Pseudomonas in 3 cases, while one patient had Staphylococcus aureus.
Risk factors associated with need of mechanical ventilation and/or mortality in H1N1 infection
Among 88 admitted patients, 14 patients required mechanical ventilation and 6 (6.8%) died. There were 5 women and 1 man among the patients who died. Six women were pregnant at time of diagnosis. Two out of six pregnant women succumbed to their illnesses with loss of foetuses due to intra uterine deaths. Two had preterm deliveries, and two were successfully discharged. They delivered at full term. Univariate analysis showed female gender, bilateral pneumonia and lymphopaenia at time of presentation as risk factors associated with need of mechanical ventilation and/or in hospital death [Table/Fig-6].
Univariate analyses of variables for need of mechanical ventilation/ mortality
| Variable, (n) | Fatal outcome no(%) | OR (95% Confidence interval) | p value |
|---|
| Gender | | | 0.004 |
| Male (44) | 2 (14.3) | 7.87(1.64-37.7) | |
| Female(44) | 12 (85.7) | | |
| Pneumonia | | | 0.002 |
| Yes (31) | 10 (71.4) | 6.31(1.78-22.35) | |
| No (57) | 4 (28.6) | | |
| CLD | | | 0.182 |
| Yes (2) | 1(7.1) | 5.61(0.33-95.52) | |
| No (86) | 13(92.9) | | |
| DM | | | 0.440 |
| Yes(12) | 1 (7.1) | 0.44 (0.052-3.71) | |
| No(76) | 13 (92.9) | | |
| Total count | | | 0.412 |
| 4000/mm3(70) | 10(71.4) | 1.714(0.468-6.27) | |
| <4000/ mm3(18) | 04(28.6) | | |
| Lymphocytes | | | <0.001 |
| <10 %(17) | 8(57.1) | 9.63(2.71-34.2) | |
| >10%(71) | 6(42.9) | | |
| Pregnancy | | | 0.221 |
| Yes (6) | 2(14.3) | 2.9(0.48-17.72) | |
| No (82) | 12 (85.7) | | |
The variables with p value <0.05 were subjected to multi variate analysis by binary logistic regression. Multivariate analysis showed bilateral pneumonia and lymphopaenia at time of presentation as independent risk factors associated with mortality or need of mechanical ventilation [Table/Fig-7].
Multivariate analysis of different variables in view of outcome (Logistic regression Method, ENTER)
| Variable | OR (95%Confidence interval) | p value |
|---|
| Gender | 5.076(0.790-32.621) | 0.712 |
| Pneumonia | 6.7 (1.3-34.5) | 0.025 |
| Lymphopenia10% | 11.7(2.258-60.9) | 0.003 |
| Pregnancy | 0.644(0.062- 35.7) | 0.712 |
Discussion
Total 495 patients reported with ILI and were tested for H1N1. 115 were positive, that accounted for 23% positivity. Study conducted by Samara T et al., [7] showed 17.35% positivity, which was similar to that in present study. Highest occurrence of H1N1 swine flu cases was in 2009-2010, while number of positive cases significantly reduced by year 2011. The cases were equally distributed in both genders. This was similar to results of earlier published Indian studies, as shown in [Table/Fig-8]. Seventy four percent of our patients belonged to age group of 19-54 years. Mean age of cohort was 31.9 years and mean age of the patients who died was 34 years. Diabetes mellitus was the most common co - existing medical condition, followed by chronic renal failure, stroke, seizure, malignancy and pregnancy. Literature showed chronic respiratory condition, chronic liver disease, chronic renal disease, diabetes and pregnancy among risk factors for H1N1 infection [7–10]. However, these risk factors were not associated with increased mortality and/or need of mechanical ventilation in the present study. This finding correlated with those of studies conducted by Samara T et al., [7] and Puvanalingam et al., [10], as shown in [Table/Fig-6]. The most common presenting symptom in present study was fever, followed by sore throat and cough, that was similar to those which were seen in other Indian studies [7–10]. In our study, 74(84%) patients recovered well and they did not have any complications. However, 14(16%) had prolonged illness and they required mechanical ventilation. Six out of 14 patients who required mechanical ventilation, died. The commonest cause of death was hypoxaemic respiratory failure with or with out acute respiratory distress syndrome and in some cases, it was multi organ dysfunction syndrome. Overall, mortality in present study was 6.8% (6/88), that was much higher than world wide mortality of 0.3-0.4% [11–14]. Another Indian study also reported mortality of 5–7%. The patients included in our study were mostly referred cases and they were more critically ill then general population level, which would have contributed to increased mortality in present study. Relative lymphopaenia is one of the risk factors for poor outcome as shown in guidelines by Winthrop University Hospital Infectious Disease Division for management of swine flu H1N1 infection [4]. We also found that lymphopaenia (lymphocytes <10%) was associated with requirement of mechanical ventilation or death in H1N1 swine flu patients. Bilateral patchy infiltrates at time of admission, was another risk factor associated with need of mechanical ventilation or mortality. We understand that bilateral pneumonia may represent secondary bacterial infection. However, bilateral pneumonia on chest X-ray might be due to bacterial pneumonia, acute respiratory distress syndrome or progressive viral pneumonia. In present series, patients were subjected to sputum gram tain and culture sensitivity if they had productive cough. Only 20 out of 73 patients who were checked, showed growth of bacteria. Fourteen out of 20 patients were mechanically ventilated and they fitted into definition of ventilator associated pneumonia. We would like to clarify that mortality in present series was crude mortality and not attributable mortality due to H1N1 swine flu infection. Five out of 6 patients who died were females; however, female gender was not an independent risk factor for mortality in multivariate analysis. Two out of 6(33%) deaths in present study occurred in pregnant women. Pregnancy is one of the important risk factors for H1N1 infection, as suggested in guidelines given by European Centre for Disease Infection and Control [11]. As seen in our analysis, studies from other countries have also reported an increased risk of influenza among pregnant women, particularly during the third trimester [5,12–14]. Although, due to racial and geological differences, it will not be appropriate to compare our results with those from western countries. We found that mortality rate among pregnant women in the U.S among H1N1 influenza cases has been around 28% [13] Samra et al., [7], Chudasma et al., [8] and Puvanalingam et al., [10] also showed increased mortality in H1N1 infection with pregnancy [7,10].
Comparison of present data with previously published Indian data
| Variable, n (%) | Samara et al., [7] May-2009 May 2010, n=52 | Chudasama et al., [8] Sept 2009 to Feb2010, n=274 | Rao et al., [9] Aug–2009 april –2010, n=20 | Puvanalingam et al., [10] Aug–2009 Jan–2010, n=442* | Present study August 2009-Dec 2011,n=88 |
|---|
| Gender | | | | | |
| Male | 32(61.5) | 141(51.5) | 6(30) | 246(55.6) | 44(50) |
| Female | 20(38.46) | 133(48.5) | 14(70) | 196(44.3) | 44(50) |
| Symptoms | | | | | |
| Fever | NA | 252(92) | 18 (90) | 95.4% | 86(98) |
| Cough | | 265(96.7) | 20 (100) | 82.23% | 76(86) |
| Dyspnea | | 146(53.3) | 10 (50) | 32.18% | 40(45) |
| Myalgia | | 59(21.5) | 05(25) | 26.7% | 22(25) |
| Age Median | 29 | 27 | NA | NA | 29 |
| <18 | | | 1 (5) | 98(17) | 11(13) |
| 18-50 | NA | NA | 18 (90) | 322(78) | 65(74) |
| >50 | | | 1 (5) | 22(5) | 12(13) |
| Mortality | 5% | 25.9% | 25% | 1.8% | 6.8% |
*Cases included were influenza like illness and not confirmed cases
NA= Not Available
Limitation
This study included only hospitalized patients of a tertiary care institute; so, analysis may not reflect the actual distribution of the cases at the population level. Due to limited resources, we could not do tests like total serum creatinine kinase and liver function tests for all the study patients, and they were restricted for intensive care unit patients. So, these tests were not included in final analysis.
Conclusion
Present study showed that out of 88 patients, 74 patients recovered well without need of MV. 14 patients required MV and among them, 6 patients died. Overall, mortality was 6.8%. Independent risk factors with mortality and/ or requiring mechanical ventilation were lymphopaenia and bilateral pneumonia at time of presentation. Pregnant women with H1N1 constituted 33% of total mortality.
*Cases included were influenza like illness and not confirmed cases
NA= Not Available