The Circle of Willis is a network of vascular channels formed anteriorly by the anterior cerebral artery, from either side. The anterior communicating artery connects these two anterior cerebral arteries. Posteriorly, the basilar artery divides into right and left posterior cerebral arteries and each joins to ipsilateral internal carotid artery through a posterior communicating artery [1].
Present study was conducted to find out variations in the anterior communicating artery, that stabilize cerebral blood flow when principle conduits fail. The anterior communicating artery displays many variations. The competence of recovery or lack of recovery after vascular occlusion partly depends upon the anatomical state of component vessel of Circle of Willis – normal or anomalous [2]. Thus, knowledge on such variations is of clinical significance.
Material and Methods
With prior permission of the ethical committee, one hundred apparently normal brain specimens were collected from formalin fixed human cadavers. The intact brains removed from the cranial cavity were again fixed in 10% formalin. The dura mater and arachnoid mater were carefully dissected out from base of the brain. The formation of Circle of Willis was observed around optic chiasma and interpeduncular fossa. Part of base of the brain was cut and it was removed in piece-meal, if it was necessary to expose the arterial circle clearly [3].
A vernier calliper graduated to measure up to 0.1 mm was used to measure the length and diameter of component vessels. The external diameters of anterior communicating artery were taken at three points, at its two ends and at the midpoint and then its average diameter was obtained. The measurements were taken twice. Any vessel with a diameter of less than 1 mm has been described as hypoplastic by various authors [4]. This definition was accepted in present study.
Gross variations in the length, diameter, course, origin, form of asymmetry, absence of component vessel (if any), branching (duplication, triplication), pattern and vessels with diameter of less than 1 mm were noted.
The course of anterior communicating artery in relation with the surrounding structures and its variations were coloured, photographed, numbered and the detailed identities of the cadavers were noted.
Observation
Among 100 cadavers, 48 were female and 52 were male cadavers. The normal pattern of anterior communicating artery was observed in 62 cadavers. The variant anterior communicating artery, which included absence, was seen in 38 cadavers. The number and types of variations seen in different sexes in present study have been shown in [Table/Fig-1,2&3] and they have been summarized diagrammatically in [Table/Fig-4].
Variations in the numbers anterior communicating artery
| Variations | Male | Female | Total |
|---|
| Absence | 4 | 4 | 8 |
| Duplication | 7 | 3 | 10 |
| Triplication | 1 | 0 | 1 |
Variations in the course anterior communicating artery
| Variations | Male | Female | Total |
|---|
| Oblique course | 2 | 0 | 2 |
| Median artery | 0 | 1 | 1 |
| In fissure | 0 | 2 | 2 |
Variations in the form of anterior communicating artery
| Variations | Male | Female | Total |
|---|
| Hypoplastic | 4 | 2 | 6 |
| Plexiform | 1 | 2 | 3 |
| Dimple | 1 | 1 | 2 |
| Fusion | 0 | 3 | 3 |
Variations of anterior communicating artery
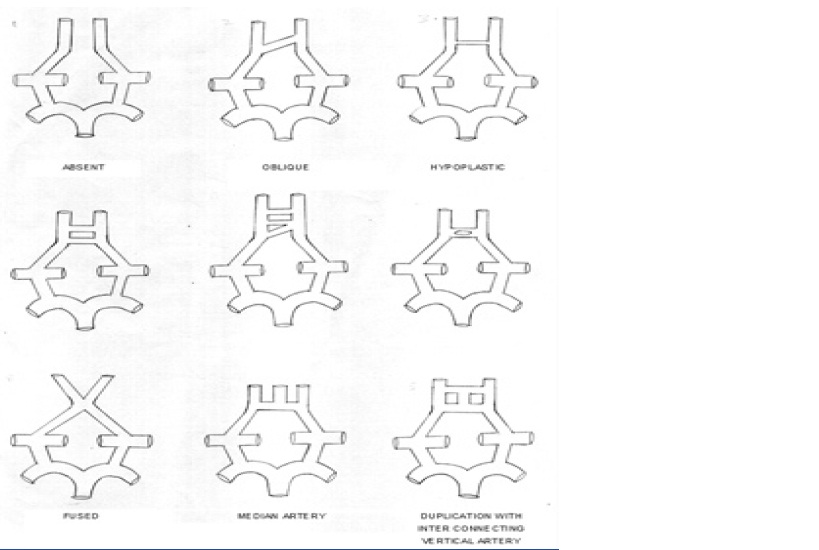
Among 100 specimens, complete absence of anterior communicating artery was found in 8 specimens, 4 male and 4 female cadavers shown in [Table/Fig-5]. In case of azygous artery, the right and left anterior cerebral arteries joined together to form a single trunk, which entered the median fissure. Thus, there was absence of anterior communicating artery in this case.
Absent anterior communicating artery

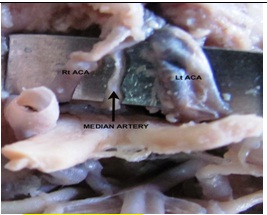
In a case where median anterior cerebral artery was present, it arose from the anterior communicating artery and entered the median fissure like the azygous artery shown in [Table/Fig-6].
Median artery arising from anterior communicating artery
In 2 males, the artery had an oblique course. In both the cases, the left end of anterior communicating artery was at a higher level than the right end shown in [Table/Fig-7].
Oblique course of anterior communicating artery

When the diameter of anterior communicating artery is less than 1mm, it is said to be hypoplastic [4]. Hypoplastic anterior communicating artery was found in [4] males and in 2 females shown in [Table/Fig-8].
Hypoplastic anterior communicating artery

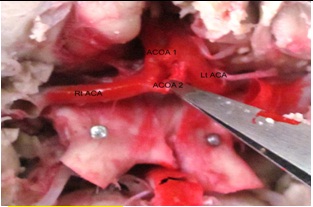
Duplication of anterior communicating artery, that is 2 anterior communicating arteries lying parallel to each other, were seen in ten specimens, in 7 males and 3 females shown in [Table/Fig-9]. In a male cadaver, the two anterior communicating arteries were parallel to each other, with an interconnecting vertical stem in between them. In one case, at the right end, both the anterior communicating arteries joined to form a single trunk in a male. Thus, the duplication was fork or Y-shaped. In one case of one male cadaver, the bifurcation was V-shaped.
Duplication of anterior communicating artery
Triplication of anterior communicating artery was seen only in one male. First two arteries were parallel to each other, but the third artery was obliquely placed. All of them were hypoplastic shown in [Table/Fig-10]. The diameter of the last artery was least among three.
Triplication of anterior communicating artery

A tuft of interconnecting network was present in between the right and left anterior cerebral arteries in 1 male and in 2 females shown in [Table/Fig-11].
Plexiform anterior communicating artery

In a female, the anterior communicating artery showed a dimple/depression on its surface shown in [Table/Fig-12]. The embryological formation of a dimple indicated an attempt of duplication. In a male, anterior communicating artery bifurcated into two branches. The distal branch of it showed a dimple on its surface.
Dimple formation in anterior communicating artery

In some cases, the right and left anterior cerebral arteries were not joined by the anterior communicating artery, but they came in close contact with each other, forming a sort fistula in between them. This variation was seen in 3 females and it was termed as a fusion.
In one case, the anterior communicating artery showed a duplication. A vertical artery connected the two branches of anterior communicating artery. The same vertical artery continued in the fissure between the right and left anterior cerebral arteries as median artery.
Due to long course of proximal segment of anterior cerebral arteries, some cases showed presence of anterior communicating artery in the fissure. Two such variants were seen in females.
Discussion
The anterior communicating artery is the artery which completes the circle of Willis anteriorly, by connecting two internal carotid arterial system. Posteriorly, the posterior communicating artery connects the vertebral arterial system with the carotid system on either side. Some workers considered the circle to be complete, even when a normal anterior communicating artery was absent and when the anterior cerebral arteries were joined together. Such circles should be considered as physiologically complete but as anatomically incomplete [5]. The variation in anterior communicating artery in the present study was observed to the extent of 38%.
In the present study, among the variations described above in [Table/Fig-13], doubling of anterior communicating artery was the most common variation, which was seen in 10% of subjects. Tripling of anterior cerebral artery was least common variation which was seen only in 1% of subjects. Same extent of a similar variation was also noted by Kanchan Kapoor [13], PN Jain [12] and Vare and Bansal [11].
Variations observed in the anterior communicating artery.
| Author | Brains examined | Absent | Fusion | Duplication | Triplication | Plexiform/ Treble |
|---|
| Windle [6] | 200 | - | 6 (3%) | 22 (11%) | - | 1 (0.5%) |
| Fawcett & Blachford [7] | 700 | 1 (0.14%) | - | 51 (7.28%) | - | 3 (0.42%) |
| Blackburn [8] | 220 | 2 (0.90%) | - | 14 (6.36%) | - | - |
| Stopford [9] | 150 | - | 5 (3.33%) | 15 (10%) | - | 2 (1.33%) |
| Von Mitterwallner [10] | 360 | 1 (0.27%) | 6 (1.66%) | 74 (20.55%) | - | 14 (3.88%) |
| Vare & Bansal [11] | 175 | 2 (1.14%) | - | 5 (2.85%) | 4 (2.28%) | - |
| P.N.Jain [12] | 144 | 1 (0.69%) | 1 (0.69%) | 19 (13.19%) | 1 (0.69%) | - |
| Kanchan Kapoor [13] | 1000 | 18 (1.8%) | - | 100 (10%) | 12 (1.2%) | 4 (0.4%) |
| Present study | 100 | 8 (8%) | 3 (3%) | 10 (10%) | 1 (1%) | 3 (3%) |
In the present study, absence of anterior communicating artery was one of the frequent variations which was observed in 8% of subjects. Fawcett and Blachford [7], Blackburn [8], Von Mitterwallner [10], Kanchan Kapoor [13], PN Jain [12] and Vare and Bansal [11] found same variation, but less frequently, to range from 0.14% to 1.8%, as compared to that in the present study.
In the present study, in 3 instances, the two anterior cerebral arteries were not joined by anterior communicating artery, but they came in close contact with each other, with a fistula formation in between them. This finding agreed with those of other workers. The incidence of this variation was similar to the observation made by Windle [6], Stopford [9]. The old author using the term fistula is not convincing Recent study done by Kanchan Kapoor [13] included this variation of fused anterior communicating artery as the absence of artery. It represents the intermediate step between a dimple formation and a duplication.
In the present study, most common variation of anterior communicating artery emerged as a duplication, which was seen in 10% of subjects. Berk [14] and Stopford [9] had reported duplication of anterior communicating artery in 9% and 7.9% cases respectively. Vare and Bansal [11] mentioned in their study, that in duplication or triplication of the vessel, the posterior most artery had a smaller size, which was similar to that which was seen in the present study. Various forms of duplications of anterior communicating artery and the incidence of this variation in present study were similar to the findings of study done by Kanchan Kapoor13. In some cases, the anterior communicating artery exhibited a dimple, which indicated an attempt of duplication. A similar case of dimpling was found in the study done by Stopford [9].
In the present study, 3% cases had persistence of plexiform pattern of anterior communicating artery, between the two anterior cerebral arteries. A similar variation with same frequency was observed by von Mitterwallner [10]. Other studies found this variation to be less frequent.
The anterior communicating artery appears in human embryo of size 18 mm, as a reticulated anastomosis between the two anterior cerebral arteries [15]. The preservation of plexus or network of vessels between the two anterior cerebral arteries exists in few adult brains, as was observed in present study.
Though rare, median artery of corpus callosum was seen to arise from anterior communicating artery and it has been described by various workers [5,11,16]. In the present study, one such case in which the median artery originated from anterior communicating artery, was noted.
Very few variations were seen in the course of vessels. Two anterior communicating arteries seen in the present study had an oblique course. In two cases, the anterior communicating artery was seen in the median fissure. This variation in the course of anterior communicating artery was associated with long and straight course of the anterior cerebral artery. Similar variations were mentioned by Vare and Bansal [11], Kanchan Kapoor [12] in their study.
Conclusion
From the present study, we can conclude that plexiform anterior communicating artery and median artery of corpus callosum are found in adults, because of persistence of embryonic pattern. Large numbers of variations were seen in anterior communicating artery (38%). Duplication was the most common variation of anterior communicating artery (10%) which was seen, followed by its absence, which was seen in 8% cases. The association of variations and the incidence of aneurysms can be interpreted in terms of haemodynamic stress caused by variations [17]. Variations of the Circle of Willis result in interruption of circulation between the internal carotid artery and vertebral artery. This forms the anatomical basis of cerebral vascular disturbances [18].