Patients with the anterior defects either due to trauma, congenital or pathological can be treated with conventional removable or fixed partial denture. The lost soft tissue structures are not replaced by the conventional treatment option. Andrews bridge is combination of both removable and fixed partial denture and fulfills all the requirements like phonetics, hygiene, aesthetics and comfort. This article describes the bar and sleeve attachment as the best treatment option in these types of defects and restores the patients satisfaction.
Congenital defects, Esthetics, Fixed bridge
Introduction
A deformed partially edentulous ridge is a major problem in the esthetic restoration of the anterior region. Deformities can be caused by traumatic extractions, trauma to the face, birth defects, apicoectomies, implant failures or advanced periodontal disease [1].
Sibert (1983) identified three basic ridge deformities Buccolingual loss of tissues(class I), Apicocoronal loss of tissues (class II) and combination of buccolongual and apicocornal loss of tissues (class III) [2].
Prosthetic dentistry involves the restoration and maintenance of oral functions, comfort, appearance and health of the patient by the replacement of missing teeth and contiguous tissues with artificial substitutes. Each restoration should be designed for the specific patient being treated. In some cases, a fixed-removable partial denture known as the Andrews bridge (Dr. James A. Andrews, Covington, La.) is superior to the conventional fixed or removable partial denture.
The fixed-removable partial denture has a pontic assembly that is removed by the patient for preventive maintenance. Primary indications for this restoration are cases where the abutments are capable of supporting a fixed partial denture but the residual ridge has been partially lost due to trauma, congenital defects or other pathologic process so that a conventional fixed partial denture would not adequately restore the patient’s missing teeth and supporting structures [3].
The success of any therapeutic treatment depends upon a variety of parameters including careful selection of suitable patients for each treatment, formation of a treatment plan and careful implementation of a gentle treatment procedure. If operator strictly adheres to these principles, any operator-induced damage can be significantly prevented [4]. Among the various restorative treatments developed for the patient with an unaesthetic edentulous space is the fixed removable partial denture. Abutment tooth stabilization is combined with a removable partial denture to resolve challenging esthetic problems [5].
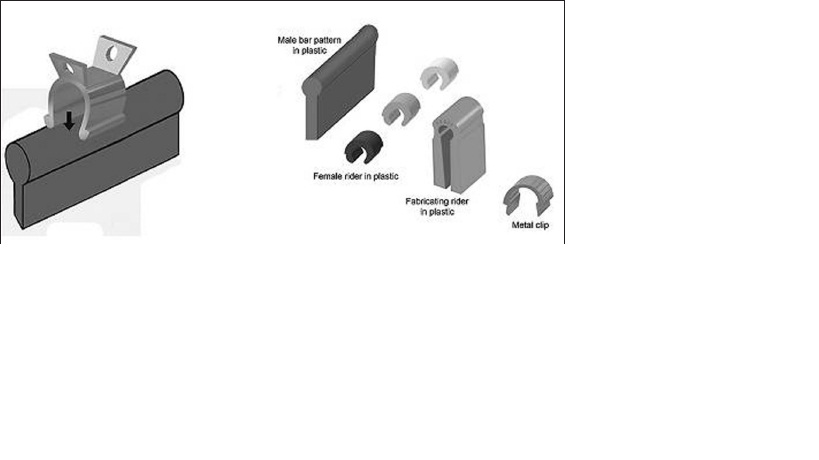
Bar attachments can be prefabricated from type-IV gold, like the original 1.6 mm Dolder bar. Prefabricated type-IV gold bars are soldered to the abutments with a low fusing solder. Other types of bars come in castable, pre-milled plastic patterns. These bars are available in 0.2° and 4° for telescopic milled restorations. The bar castings should only be made with hard alloys. A minimum Vickers hardness of 200 and at least 95,000 psi ultimate tensile strength is required. Non-precious alloys are contraindicated for implant reconstruction.
Bar clips or riders are available in different materials and configurations. The metal clips and riders are fully adjustable. Plastic Hader/EDS clips are non-adjustable, but they can easily be replaced at chair side.
Bar attachments can be classified by their cross-sectional shape as round, egg-shaped and parallel-sided U-shaped. Bars that are resilient, providing vertical resiliency, hinge resiliency or both, are termed bar joints. Bars that are non-resilient are termed bar units [6].
Case report 1
A 20-year-old girl reported to Department of Prosthodontics, with a removable partial denture in upper right anterior region. She was not happy with the prosthesis and wanted a replacement with a fixed prosthesis. She gave history of right lateral incisor extraction at the time of surgery for cleft palate and lip correction. There was severe bone loss with depressed lip support [Table/Fig-2]. The abutment teeth had sufficient support for a fixed prosthesis. Because of the severe ridge defect in anterior region a fixed partial denture couldn’t be planned as it would have lead to an elongated pontic and poor hygiene maintenance. So Bar and Sleeve attachment was best option for esthetic, hygiene concerns and also fulfilled patients requirement.
Case report 2
A 32-year-old male patient reported to the Department of Prosthodontics with complaint of missing teeth in left anterior region of mouth.He lost his teeth in bike accident eight months back, there was bone loss in affected region, the rest of the supporting abutments were in good condition [Table/Fig-3].
The conventional fixed partial denture would not have adequately replaced the teeth and the supporting structures so combination of fixed and removable partial denture (Andrews bridge) was the best treatment option.
The defect required the prosthesis to restore not only the missing teeth but a large area of supporting structures as well. The appropriate bar was selected in both cases (case1 and case 2) from the preformed curvatures available using diagnostic casts. The bar followed the residual ridge and was positioned in the approximate center of the replacement teeth.
Endodontic treatment followed by crown preparation of the abutments was done as used in making fixed partial denture
Alginate impressions were made of maxillary and mandibular arches for making fixed portion of the designed bridge
Provisional restorations were made and cemented on the prepared abutments and a provisional removable partial denture was made.
The bar was placed in the pontic section in relation to crown and ridge without interference on the labial and lingual surface
There was increased clearance between the bar and the tissue. Bar was positioned so that path of withdrawal of removable segment was divergent from displacing forces exercised on fixed portion.
The pattern was invested, cast and finished, then a plastic sleeve was placed on the bar, the cast was reproduced in stone and the nylon retentive clasps were transformed
Acrylic teeth were selected according to patients age, sex and personality and final approval of the patient was taken after the try-in procedure.
The shade of abutment teeth was selected, porcelain was added to the retainers and finally glazed
The prosthesis was processed and polished, the flange prosthesis was placed in the mouth, the tissue adaptation and esthetics was checked, after patients confirmation the abutment retainers were cemented.
The bridges were delivered and patient was instructed in removing and inserting the pontics, also oral hygiene instructions were given.
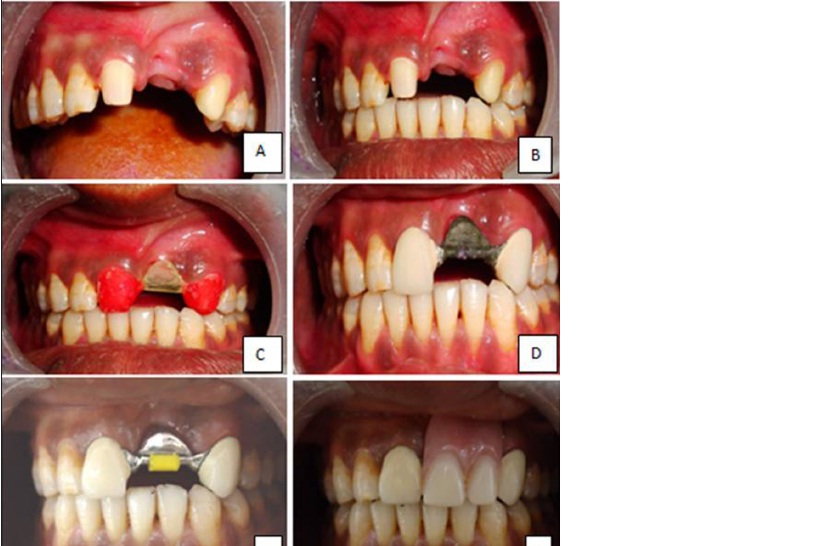
A. Anterior bone loss. B. Resin pattern coping with bar C. Try in. D.Resin pattern coping with bar. E. Final prosthesis. F. Removable prosthesis insertion
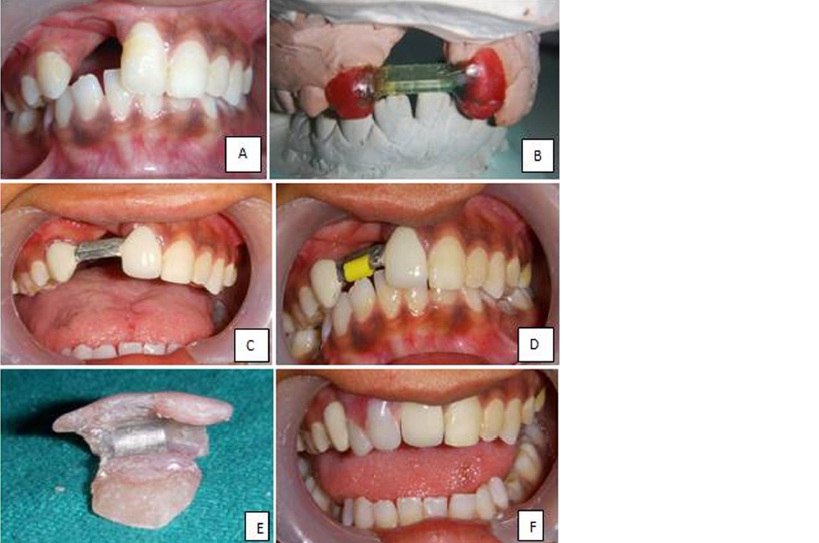
A. Prepared Teeth. B. Anterior Bone loss. C. Resin pattern coping try in. D. Try in. E. Cementation with clip on bar. F. Removable prosthesis insertion
Discussion
During treatment planning case selection was the important part of the treatment as there was severe bone loss in both cases. The esthetic replacement of anterior teeth is a difficult challenge, especially in the maxillary arch. This situation can be further complicated by the presence of a ridge deformity. These anatomic defects may seriously compromise the esthetics of the final restoration [1]. All the treatment choices were explained to the patient, after the patients final decision the Andrews bridge was the treatment of choice.
Andrews bridge has both fixed and removable properties. Andrew’s system provides maximum aesthetics and optimum phonetics in cases involving considerable supporting tissue loss, jaw defects and when alignment of the opposing arches and/or aesthetic arch position of the replacement teeth create difficulties. Another favourable criterion of the Andrew’s bar system is that it can be removed by the patient for hygienic access to the abutments and surrounding tissues [7]. The Andrews bridge is more stable and retentive because it is completely tooth borne and the occlusal forces are also directed towards the long axis of the supporting teeth [3].
Compared to a conventional removable partial denture, the fixed-removable partial denture is more stable because it is totally tooth-borne and the occlusal forces are directed more along the long axes of the abutment teeth.
Compared to a conventional fixed partial denture, the pontic teeth are arranged during the esthetic try-in appointment. The flange of the pontic assembly is contoured to improve comfort, esthetics, and phonetics, and to resist possible torque during function. Moreover, in contrast to conventional fixed partial dentures, the pontic assembly is removed to facilitate hygiene procedures and may be relined as the ridge resorbs [3].
The bar and sleeve technique have evolved to produce whole new classes of prosthesis. Twin Andrews bars and a double track sleeve allow for a tissue supported, unilateral, free end saddle partial denture. It eliminates maintenance and phonetic problems of header bar retained partial denture. Andrews bridge have been marvelously adapted to implant prosthesis [8].The Andrew’s bar system provides maximum aesthetics, Maximum hygiene, optimum loading conditions, minimum trauma to the Soft tissues, incomparable fit and is very economic [7].
[1]. H Abrams, RA Kopczyk, AL Kaplan, Incidence of anterior ridge deformities in partially edentulous patients.J Prosthet Dent 1987 57:191-94. [Google Scholar]
[2]. JS Seibert, Reconstruction of deformed partially edentulous ridges , using full thickness graft. Part 1 Technique and wound healingCompend Cont Ed Gen Dent. 1983 4:437-53. [Google Scholar]
[3]. A Mueninghoff L, MH Johnson, Fixed-removable partial dentureJ Prosthet Dent 1982 48:547-50. [Google Scholar]
[4]. E Moslehifard, mplant Dentistry – The Most Promising Discipline of Dentistry. 2011 :1-29. [Google Scholar]
[5]. J Everhart R, E Cavazos, Evaluation of a fixed removable partial denture: Andrews Bridge SystemJ Prosthet Dent 1983 50:180-84. [Google Scholar]
[6]. H Shafie, G Obeid, Principles of attachment selection for implant-supported overdentures and their impact on surgical approaches. Shroms19(6):1-36. [Google Scholar]
[7]. M Sadig W, Bone Anchored Andrew’s Bar System-A Prosthetic AlternativeCairo Dental Journal 1995 11:11-15. [Google Scholar]
[8]. A Andrews J, F Biggs W, The Andrews Bar-Sleeve Retained Bridge –a case reportDentistry Today 1999 18(4) [Google Scholar]