Utility of Diagnostic Ultrasound in Evaluating Fracture Healing
Sushil G. Kachewar1, Devidas S. Kulkarni2
1 Associate Professor, Department of Radiology, Rural Medical College (RMC), PIMS, Loni, India.
2 Professor, Department of Radiology, Rural Medical College (RMC), PIMS, Loni, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sushil G. Kachewar, Associate Professor, Department of Radiology, Rural Medical College (RMC), PIMS, Loni, India.
Phone: 9921160357,
E-mail: sushilkachewar@hotmail.com
With increase in population, modes of transportation and a fast pace of life, an individual’s chances of accident and thereby chances of getting fractured have increased significantly. Fracture has thus become a significant factor contributing to morbidity and mortality. To resume a normal life, after one suffers from a fracture is also an ordeal. The transition appears smooth if the fracture healing goes on in a smooth manner as is expected through its routine stages of reactive phase, reparative phase and remodeling phase. But if in this chain something goes wrong or some factors are not optimum upto the mark, then the process becomes unsuccessful and the repair is either partial or directionless. It is therefore very vital to confirm whether or not the callus which bridges the fractured fragments is healthy or not. Here in lies the role of imaging as it can show the status of callus without disturbing it. What complicates the picture is that a callus might not be well demonstratable unless it mineralizes or calcifies. An imaging modality like ultrasound therefore stands out as it can show the state of callus in its different stages. This article aims at demonstrating how ultrasound- a non invasive diagnostic imaging modality can give precise information about the progress of fracture healing and thereby aid in management of fractures, so that an individual can return back to normal productive lifestyle. This preliminary study highlights the spectrum of fracture healing as seen on ultrasound.
Fracture, Healing, Ultrasound, Callus, Mineralization, Vascularization
Introduction
High mortality and morbidity has been attributed to fractures of the human body. The incidence of fractures is on rise due to changes in socio-economic behaviors [1]. The medical, economical and social effects of fractures are manifold [2]. Disability primarily results from persistent pain and limited physical mobility. Hence the aim of the patient as well as the treating specialist is to return the patient back to the activities of daily living independently as soon as possible. But if the process of fracture healing is not appropriate it may lead to complications like delayed healing, non- healing or even fibrous union. Therefore, to correctly detect whether the process of healing is in proper direction or not is the main requirement. Non-invasive diagnosis is possible with the help of plain radiography, CT scan, MRI scan as well as Ultrasound scan. Ultrasound being cheap and a portable (bedside) modality has the best potential for evaluating the process of fracture healing.
The Mechanisms of Fracture Healing
The process of bone healing following a fracture goes through various stages. Numerous phases of recovery facilitate the proliferation and protection of the areas surrounding fractures and dislocations. The length of the process depends on the extent of the injury, and usual margins of two to three weeks are given for the reparation of most upper bodily fractures; anywhere above four weeks given for lower bodily injury [3–6].
Entire regeneration of the bone also depends on the angle of dislocation or fracture. Bone marrow within the fracture has healed two or fewer weeks before the final remodeling phase.
The role of immobilization and surgery is just to facilitate healing; as ultimately healing is through the natural physiological processes. There are three major phases of fracture healing. In the first phase (Reactive Phase) there is he fracture followed by inflammatory cell influx which is then followed by granulation tissue formation. In the second phase (Reparative Phase) calcifications are laid down in the callus which leads to formation of cartilage callus. This is then modifies into lamellar bone deposition. In the third phase (Remodeling Phase), the bone returns to its normal morphology and becomes fully functional.
Plain Radiographs can show only the late second and third phases of fracture healing as shown in [Table/Fig-1]. Although plain radiography is a modality of choice in follow up of patients of fracture, it is woefully silent for the first two stages. Higher imaging modalities like CT and MRI scan might not always be feasible and available.
Fresh fracture in R femur and old united fracture in L femur
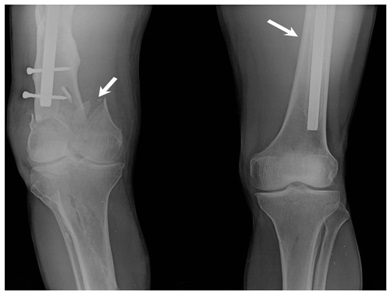
Ultrasound stands true to this test. It can non-invasively image all the three phases of fracture healing but can also pinpoint any drawbacks in healing process. Moreover, it can used repeatedly and even has a huge bedside potential. Ultrasound can demonstrate all these phases and hence is vital for diagnosis and follow up.
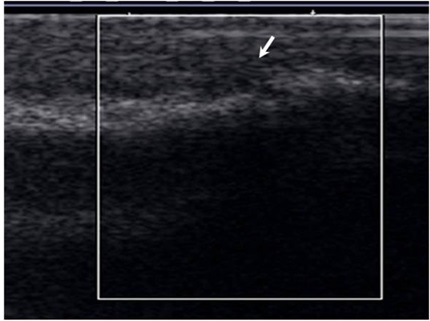
In the reactive phase, following a fracture, blood is seen within the tissues adjacent to the injury site. Soon the extra vascular blood cells form a blood clot, known as a hematoma [Table/Fig-2]. All of the cells within the blood clot degenerate and die; except the fibroblasts which survive and replicate and form a granulation tissue. This phase last for 48-72 hours.
USG at fracture site showing hematoma formation
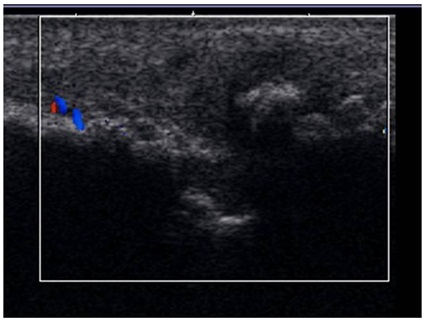
Then follows of stage of vascularized callus formation [Table/Fig-3]. Presence of abundant vascularity in callus indicates a healthy callus. This phase lasts for 2-4 weeks.
USG at fracture site showing vascularization in callus
In the reparative phase, the cells of the periosteum replicate and transform into chondroblasts which form hyaline cartilage. The periosteal cells distal to (further from) the fracture gap develop into osteoblasts which form woven bone. The fibroblasts within the granulation tissue develop into chondroblasts which also form hyaline cartilage [Table/Fig-4]. These two new tissues grow in size until they unite with their counterparts from other parts of the fracture. Then there is the replacement of the hyaline cartilage and woven bone with lamellar bone. The replacement process is known as endochondral ossification with respect to the hyaline cartilage and bony substitution with respect to the woven bone. This phase extends from 4-8 weeks.
USG at fracture site showing cartilage and bone formation and callus remodeling
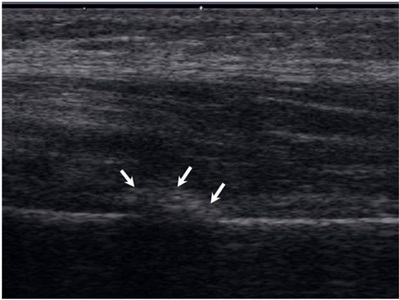
In the remodeling phase [Table/Fig-4], the trabecular bone is replaced with compact bone, such that the fracture callus is remodeled into a new shape which closely duplicates the bone’s original shape and strength. The remodeling phase takes 3 to 5 years depending on factors such as age or general condition.
In addition to demonstrating these various phases of fractures healing, Ultrasound can also distinctly show the complications of fracture healing like Delayed Union (USG-Poor blood supply or infection at fracture site even after the expected period of healing), Non-Union (USG-Bone loss or wound contamination at fracture site) and the Fibrous Union (USG-Fibrous tissue seen as hypoechoic structure as against the callus at fracture site).
The Health Impacts of Calcifications in Callus
The presence of calcifications in the callus at fracture site is a sure sign that the callus is getting mineralized and progressing successfully towards a complete recovery. Plain Radiograph cannot identify this phase as these initial calcifications are very tiny and hence are unseen on radiographs. Moreover it has been shown in an experiment study that x-ray appearances of healing can be prevented by a failure of calcification even though a good organic callus is present [7]; this can only be detected on Ultrasound.
Ultrasound is the best as it identifies even the tiniest of the tiny calcific specks and provides reassurance to the patient as well as the specialist managing the case. As ultrasound can visualize developing callus even before radiographic changes are evident, it can therefore be utilized to assess the changes of bone healing [8]. The presence of a hyperechoic ultrasound signal from the fracture sight was found to have a 100 percent correlation with the presence of hard fracture callus biopsy tissue [9].
In addition to diagnosing the fracture healing, Ultrasound can infact accelerate the fracture-repair process by inducing conformational changes in the cell membrane and thus altering ionic permeability and second messenger activity [10, 11]. Ultrasound also stimulates angiogenesis, thus increasing blood flow to the fracture site and inherently delivering the key components, such as growth factors and cytokines that are necessary for the normal healing process [12].
Color-Doppler US and the spectral analysis provides additional functional data, on bone callus and newly formed bone vascularization [13]. In the patients with positive fracture evolution it has been observed that the caliber of afferent vessels progressively increases, their number decreases and branches appear. The RI progressively increases, up to similar values to those of nutrient vessels (.36 to .90). Within the second month of fracture, a telesystolic notch appears: this indicates a muscular tunic in the vessel wall, meaning a mature, and no longer a newly formed vessel. The normal evolution of bone healing may be interrupted by several mechanical and biohumoral factors which reportedly act in a similar way by reducing the number of vessels and increasing peripheral resistance in residual vessels because of fibrosclerotic involution of bone healing. Color-Doppler US permits noninvasive, repeatable and nearly real-time monitoring of bone fracture healing, which suggests this technique could be used: -to assess the results of treatment changes (e.g., loading, external fixator adjustments); -to study the definitive callus; -for the medicolegal assessment of delayed bone healing and of pseudoarthrosis; -for real-time treatment planning, according to color-Doppler findings, and to monitor treatment results.
[1]. Zain Elabdien BS, Olerud S, Karlström G, Smedby B, Rising incidence of hip fracture in Uppsala, 1965-1980Acta Orthop Scand 1984 55(3):284-9. [Google Scholar]
[2]. Thomas TG, Stevens RS, Social effects of fractures of the neck of the femurBr Med J 1974 3(5928):456-8. [Google Scholar]
[3]. Brighton Carl T, Hunt Robert M, Histochemical localization of calcium in the fracture callus with potassium pyroantimonate: possible role of chondrocyte mitochondrial calcium in callus calcificationJournal of Bone and Joint Surgery 1986 68-A(5):703-15. [Google Scholar]
[4]. Brighton Carl T, Hunt Robert M, Early histologic and ultrastructural changes in medullary fracture callusJournal of Bone and Joint Surgery 1991 73-A(6):832-47. [Google Scholar]
[5]. Brighton Carl T, Hunt Robert M, Early histologic and ultrastructural changes in microvessels of periosteal callusJournal of Orthopaedic Trauma 1997 11(4):244-53. [Google Scholar]
[6]. Ham Arthur W, William R Harris, Repair and transplantation of boneThe biochemistry and physiology of bone 1972 New YorkAcademic Press:337-99. [Google Scholar]
[7]. Ham AW, Tisdall FF, Drake TGH, Experimental non-calcification of callus simulating non-unionThe Journal of Bone & Joint Surgery 1938 20:345-52. [Google Scholar]
[8]. Craig Joseph G, Jacobson Jon A, Moed Berton R, Ultrasound of fracture and bone healingRadiologic Clinics of North America 37 4:737-51. [Google Scholar]
[9]. Moed BR, Kim EC, van Holsbeeck M, Schaffler MB, Subramanian S, Bouffard JA, Ultrasound for the early diagnosis of tibial fracture healing after static interlocked nailing without reaming: histologic correlation using a canine modelJ Orthop Trauma 1998 12(3):200-5. [Google Scholar]
[10]. Ryaby JT, Mathew J, Pilla AA, Duarte-Alves P, Low-intensity pulsed ultrasound modulates adenylate cyclase activity and transforming growth factor beta synthesis. In: Brighton CT, Pollack SR, editorsElectromagnetics in medicine and biology 1991 San FranciscoSan Francisco Press:95-100. [Google Scholar]
[11]. Ryaby JT, Mathew J, Duarte-Alves P, Low intensity pulsed ultrasound affects adenylate cyclase activity and TGF-b synthesis in osteoblastic cellsTrans Orthop Res Soc 1992 7:590 [Google Scholar]
[12]. Rawool D, Goldberg B, Forsberg F, Winder A, Talish R, Hume E, Power Doppler assessment of vascular changes during fracture treatment with low intensity ultrasoundTrans Radiol Soc North Am 1998 83:1185 [Google Scholar]
[13]. Bottinelli O, Calliada F, Campani R, Bone callus: possible assessment with color Doppler ultrasonography. Normal bone healing processRadiol Med 1996 91(5):537-41. [Google Scholar]