Introduction
World-wide, preterm delivery is associated with substantial short as well as long term physical, emotional, psychological or financial impacts. Preterm labour is defined as delivery before 37 completed weeks of pregnancy. Every year, an estimated 15 million babies are born preterm and the number is rising [1]. In the United States in 2011, 23,910 infants died in their first year of life [2]. Preterm birth has been implicated in approximately two thirds of these deaths [3]. Significant progress has been made in the case of management of premature infants, but not in reducing the prevalence of preterm birth. Preterm birth is the leading cause of newborn deaths and also the leading cause of death in children under 5 years of age [1]. Three quarters of them could be saved with current, cost effective interventions, even without intensive care facilities.
The cause of preterm labour is in many cases elusive. There are many postulated causes which makes reduction of preterm labour a challenging preposition. Infection has been suggested to strongly associate with preterm [4]. Current data suggest microbial invasion of the reproductive tract is sufficient to induce infection mediated preterm birth-more specifically; there is ongoing subclinical infection [5].
A large proportion of early spontaneous preterm deliveries are associated with upper genital tract infections and most patients show little or no sign of infection [6]. The earlier the onset of preterm labour, the greater is the likelihood of documented amniotic fluid infection [7]. Periodontal disease -Gum inflammation is a chronic anarobic inflammation that affects as many as 50% of prgnant women in the United States. Vergnes and Sixou performed a meta analysis of 17 studies and concluded that periodontal disease was significantly associated with preterm birth [8]. Bacterial vaginosis has been associated with spontaneous abortion, preterm labour, preterm premature rupture of membranes, chorioamnionitis and amniotic fluid infection [9]. Other factors-that include preterm labour are high blood pressure, preeclampsia, maternal diabetes, asthma, thyroid disease, heart disease [10].
Preterm premature rupture of membranes (PPROM) defines spontaneous rupture of fetal membranes before 37 completed weeks and before labour onset [5].Current study also included PPROM as one study group as infection is a known risk for this of PPROM [11]. Attempts to identify biomarkers for preterm labour remains a constant endeavor.
Ferritin is an acute phase reactant as it increases during inflammation [12]. This study aims to determine whether serum ferritin levels which may be raised in the setting of any infective process could be used as a marker of spontaneous preterm labour or PPROM.
Ferritin level can be increased in cases of excess iron storage in the body. Transferrin level and TIBC will be low in such conditions. The parameters included in the study are Serum ferritin, transferrin, iron and TIBC. When ferritin is increased in the study group relative to the control group with comparable serum iron, TIBC and transferrin in both study group and control group, it can be said that the increase is due to infection and not a reflection of iron status.
Objectives
Objectives were to compare the ferritin levels in 50 patients of PPROM, 50 patients of spontaneous preterm labour and 50 pregnant women matching with haemoglobin and same gestational age. And also, to estimate serum iron, TIBC and transferring saturation percent in the above 3 groups.
Study is a Descriptive cross sectional study (Comparative study). The duration of the study was from March to August 2013. Study setting was Labour room and OPD of the Department of Obstetrics and Gynaecology, Govt. Medical College, Kottayam. As well as in the Department of Clinical Biochemistry, Govt. Medical College, Kottayam.
Inclusion criteria
The first 50 patients of spontaneous preterm labour, 50 patients with preterm premature rupture of membranes and 50 pregnant women serving as controls comprising of subjects who did not have preterm labour or preterm premature rupture of membranes from March 2012 to August 2013 were taken into the study. Controls i.e. the group with no preterm labour or preterm premature ruptures of membranes were matched for Hb percent and the period of gestation with the study group.
Exclusion criteria
Subjects with anemia, iron overload state, pre-existing chronic infective disease, multiple pregnancy, polyhydramnios, diabetes mellitus, subjects with obvious genital tract infections or infections anywhere else in the body, liver disease, renal disease, malignancy and any known risk factor were excluded from the study. Alcoholics, smokers and subjects with uncertain gestational age were also excluded from the study
Procedure: Serum Ferritin and transferrin were estimated using immunoturbidimetric method [13,14]in BECKMAN COULTER AU 480. Serum iron and UIBC were estimated using photometric using ferene. TIBC was calculated by adding iron and UIBC. 3ml blood was collected from the obstetric OPD for the control group. For the PPROM and spontaneous preterm labour, blood was collected from the labour room. Blood collection tubes were transferred to the lab and centrifuged to convert it to serum. Then it was estimated in AU 480.
Statistical Analysis
The data was properly coded and was entered in Microsoft Excel. The statistical analysis was done using software SPSS 16.0. Mean, standard deviation and standard error were calculated for each parameter (serum ferritin, serum iron, serum transferrin, TIBC).
Significance of difference in the means of different parameters (serum ferritin, serum iron, serum transferrin, TIBC) between the pregnant women (preterm) in the 3 groups were found out using ANOVA. Significance of difference in the means of different parameters (serum ferritin, serum iron, serum transferrin, TIBC) between the control group and pregnant women with spontaneous preterm labour and preterm premature rupture of membranes were found out by using a post-hoc test (Tukey test). A p-value of < 0.05 was considered significant.
Serum Ferritin levels in the study population
| Group (n) | Mean(microgram/L) | Standard deviation | Standard error | ANOVA |
|---|
| Control (50) | 29.26 | 14.44 | 2.04 | F=4.24 |
| PPROM (50) | 40.38 | 11.41 | 1.61 |
| Spontaneous preterm (50) | 36.11 | 10.79 | 1.53 |
Results
The subjects in the study were in the age group of 21 to 35 years with a mean age of 26.64 years and a standard deviation of 2.836
1) Ferritin
Difference in the means of serum ferritin between the pregnant women (preterm) in the 3 groups was found out using ANOVA and was found to be significantly different. (F statistic: 4.24 and p-value: 0.012). To find out which groups were significantly different a post hoc test (Tukey test) was applied and it was found that there was significant statistical difference in the mean ferritin values between the control group and PPROM group as indicated by the p-value of 0.012.There was no significant statistical difference in the mean ferritin values between the control group and spontaneous preterm labour group as indicated by a p-value of 0.180.
2) Transferrin
Difference in the means of serum transferrin between the pregnant women (preterm) in the 3 groups was found out using ANOVA and was not found to be significant with a (F statistic:1.78 and p-value: 0.17).
3)Iron
Difference in the means of serum iron between the pregnant women (preterm) in the three groups was found out using ANOVA and was not found to be significant with a F statistic of 2.04 and a p-value: 0.134.
4) Tibc
Significance of difference in the means of TIBC between the pregnant women (preterm) in the 3 groups was found out using ANOVA and was not found to be significant with a (F statistic: 0.087 and p-value: 0.917).
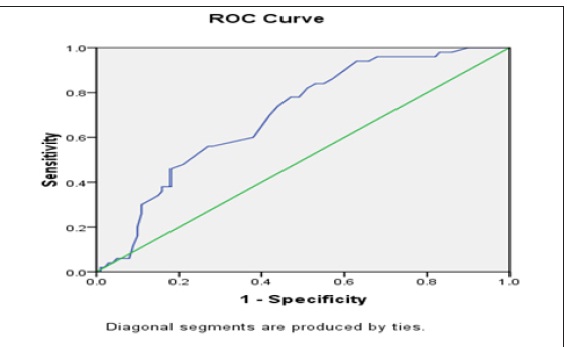
[Table/Fig-2] Receiver operating characteristic curve showing serum ferritin levels and PPROM ROC CURVE .
The ROC curve [Table/Fig-2] of serum ferritin in diagnosis of PPROM was found to be significant with a p-value of 0.0010. (95% confidence interval 0.616-0.784), a standard error of 0.043 and area under the curve 0.70.
Discussion
The mean values of serum ferritin in the control, PPROM and women with spontaneous preterm labour were 29.26, 40.38 and 36.11microgram/L respectively. The standard deviation of ferritin in the control, PPROM and women with spontaneous preterm labour were 14.44, 11.41 and 10.79. There is a significant statistical increase in serum ferritin in the PPROM group when compared to the control group (p-value < 0.05).Study conducted by Bhawna singh et al., showed ferritin a potential biomarker in the prediction of preterm delivery [15]. In the study conducted by Saha et al., mean ferritin values in the control group, PPROM and spontaneous preterm labour were 8.69± 3.7, 29.4± 28.41 and 23.24± 12.13 microgram/L respectively [16]. In that study there was significant difference between control group and PPROM as well as with spontaneous preterm labour. But in the present study there is significant statistical difference between control group and PPROM but no significant difference between control group and spontaneous preterm labour.
The high values in the serum ferritin levels in the PPROM cases could be due to infection associated with PPROM cases and there is compelling evidence that infection causes a significant proportion of PPROM cases. The inflammatory response that leads to membrane weakening is currently being defined. A number of studies have been done to ascertain the incidence of infection induced PPROM. Bacterial cultures done by Goncalves support a role for infection in a significant proportion. A review of 18 studies comprised of almost 1500 women with PPROM found that in a third, bacteria were isolated from amniotic fluid [5]. So, the high ferritin level in the PPROM group is most likely due to latent chorioamnionitis.
In pregnancy there is change in vaginal pH which may result in vagino cervical infection. This follows bacterial colonization and macrophage infiltration at the chorion decidual interface and ferritin is produced as part of acute phase response. Brailsford proposed that the increased extracellular ferritin has an important role in host defense against bacteremia by stimulating oxidative metabolism [17].
The high serum ferritin level in the PPROM group is thus most likely a part of ‘acute phase reaction’ to a subclinical genital infection or inflammation. So, serum ferritin may be used a marker of PPROM cases and may help the physicians to anticipate it. In the present study, there was no significant statistical difference in the mean ferritin values between the control group and spontaneous preterm labour group (p-value >0.05). A retrospective study by Gopal et al., also had shown no relation between serum ferritin levels and spontaneous preterm labour [18]. Even though there is widespread suspicion that subclinical infection is a common accompaniment and cause of spontaneous preterm labour, serum ferritin levels was not significantly raised in my study group of spontaneous preterm labour cases. So it shows spontaneous preterm labour may be due to multifactorial causes than attributing only to subclinical infection. A study conducted by Goncalves showed that microorganisms are not recovered from the amniotic fluid in all women with spontaneous preterm labour [19]. In fact, the incidence of positive cultures in women with spontaneous preterm labour averages only 15% [19]. Since the serum ferritin levels are not significantly raised, it cannot be used a marker of spontaneous preterm labour. Thus serum ferritin estimation may not have much role in anticipating spontaneous preterm labour and won’t be of much help to obstetricians to take an appropriate action to prevent it. This is contradictory to the findings of Saha et al., [16].
The mean values of serum iron in the control group, PPROM group and women with spontaneous preterm labour in the present study were 111.14, 129.1 and 117.16 microgram/dL respectively. The standard deviation of iron in the control, PPROM and women with spontaneous preterm labour were 62.48, 35.94 and 30.07 respectively. There was no significant statistical difference in the mean iron values of women with PPROM and spontaneous preterm labour when compared to the control group (p-value > 0.05).
The lack of significant statistical difference may be due to the wide range in serum iron levels and day to day variations in serum iron. Serum iron values in an individual can vary within a single day or from day to day [20]. However, in the present study, there was mild increase in the serum iron values in the PPROM cases. This could be due to covert process of infection in PPROM cases which is known to raise serum iron as a result of tissue damage.
The mean transferrin in the control group, PPROM group and women with spontaneous preterm labour were 295.92, 278.96 and 290.48milligram /dL respectively. The standard deviation of transferrin in the control, PPROM and women with spontaneous preterm labour were 48.41, 49.18 and 39.37 respectively. The serum transferrin was higher in the control group and women with spontaneous preterm labour, but this difference was not statistically significant (p-value > 0.05). The serum transferrin levels were slightly less in the PPROM cases when compared to the control group and women with spontaneous preterm labour cases but there was no statistical significance (p-value >0.05). This may be because transferrin is a negative acute phase reactant [21] and is found to decrease in inflammation or infection as in case of PPROM cases.
The mean TIBC in the control group, PPROM group and women with spontaneous preterm labour were 423.24, 416.74 and 421 microgram/dL respectively. The standard deviation of TIBC in the control, PPROM and women with spontaneous preterm labour were 112.19, 58.08 and 53.25 respectively. There was no significant statistical difference in the mean TIBC values of PPROM group and women with spontaneous preterm labour when compared with the control group (p-value >0.05). It is consistent with the findings of Aysha Siddika [22].
5 pregnant women in the control group had transferrin saturation <16% and serum ferritin <150microgram/L which indicates iron deficiency and 2 in the study group had transferrin saturation <16% and serum ferritin <150microgram/L. 6 in the control group had transferrin saturation <16% and serum ferritin >150microgram/L and 2 in the study group had transferrin saturation <16% and serum ferritin >150 microgram/L.
ROC curve was done to find out the role of serum ferritin in predicting PPROM and was found to be statistically significant. The level of ferritin at which it had maximium sensitivity with a logical specificity was for 35.5. For a value of 35.5 microgram/L sensitivity was 74% and specificity was 66%. So, a cut off value of serum ferritin 35.5 microgram/L would be ideal to predict the probability of PPROM.
Thus serum ferritin may be used as a marker of PPROM cases and may help the obstetricians to anticipate it by checking serum ferritin levels. But serum ferritin cannot be used as a marker of spontaneous preterm labour cases and is not of much use for the obstetricians as a screening test to prevent it. Spontaneous preterm labour may be due to multifactorial causes and cannot be attributed only to infection.
Conclusion
Serum ferritin was significantly elevated in PPROM cases when compared to the control group of women with same gestational period. Serum ferritin was not significantly elevated in spontaneous preterm labour cases when compared to the control group. Serum transferrin, iron and TIBC were also not significantly elevated in the study group when compared to control group.So serum ferritin may be used as a marker for PPROM but not for spontaneous preterm labour.
Recommendations
The present study recommends the use of serum ferritin as a marker for PPROM and could be used to prevent complications by obstetricians worldwide. The current study has helped to evolve a cut off value of 35.5microgram/L of serum ferritin for predicting the PPROM cases.
[1]. Preterm birth. [online]. 2004 Available from: URL: http://www.who.int/mediacentre/factsheets/fs363/en/ [Google Scholar]
[2]. S Hamilton, Y Oomomian, G Stephen, O Shynlova, CL Tower, A Garrod, Macrophages infiltrate the human and rat decidua during term and preterm labour: evidence that decidual inflammation precedes labour.Biol Reprod 2012 86(2):39 [Google Scholar]
[3]. TJ Mathews, MF Macdorman, Infant mortality statistics from the 2009 period inked birth/infant data setNatl Vital Stat Rep 2013 61(8):1-27. [Google Scholar]
[4]. J Burdet, AP Rubio, AL Salazar, ML Ribeiro, C Ibarra, AM Franchi, Inflammation, infection and preterm birthCurr Pharm Des. 2014 20(29):4741-78. [Google Scholar]
[5]. FJ Cunningham, KJ Leveno, SL Bloom, CY Spong, JS Dashe, BL Hoffman, 2014 24th EditionNew YorkWilliams Obstetrics Mc Graw Hill Education:838-39. [Google Scholar]
[6]. RS Gibbs, The relationship between infections and adverse pregnancy outcomes: an overview.Ann periodontal. 2001 6(1):153-63. [Google Scholar]
[7]. RL Goldenberg, JC Hauth, Chorio-decidual infection and preterm birthNutr Rev 2002 :60-S19.. [Google Scholar]
[8]. JN Vergnes, M Sixou, Preterm low birth weight and maternal periodontal status: A meta analysis.Am J Obstet Gynaecol 2007 196(135) [Google Scholar]
[9]. H Leitich, B Bodner-Adler, M Brunbauer, A Kaider, C Egarter, P Husslein, Bacterial vaginosis as a risk factor for preterm delivery: a meta-analysis..Am J Obstet Gynecol. 2003 189(1):139-47. [Google Scholar]
[10]. RL Goldenberg, JF Culhane, JD Iams, Preterm birth 1: Epidemiology and causes of preterm birth.Lancet. 2008 371(75) [Google Scholar]
[11]. NA Riyami, IA Ruheili, FA Shezaw, MA Khabori, Extreme Preterm Premature Rupture of Membranes: Risk Factors and Feto Maternal OutcomesOman Med J. 2013 28(2):108-11. [Google Scholar]
[12]. G Beck, TW Ellis, GS Habicht, SF Schluter, JJ Marchalonis, Evolution of the acute phase response: iron release by echinoderm (Asteriasforbesi) coelomocytes, and cloning of an echinoderm ferritin moleculeDevelopmental and comparative immunology. 2002 26(1):11-26. [Google Scholar]
[13]. M Worwood, The labouratory assessment of iron status-an updateClin Chim Acta. 1997 259:3-23. [Google Scholar]
[14]. F Dati, G Schumann, L Thomas, F Aguzzi, S Baudner, J Bienvenu, Consensus of a group of professional societies and diagnostic companies on guidelines for interim reference ranges for 14 proteins in serum based on the statndardisation against the IFCC/BCR/CAP reference material (CRM 470).Eur J Clin Chem Clin Biochem. 1996 34:517-20. [Google Scholar]
[15]. B Singh, B Goswami, N Gupta, AD Bajaj, V Mallika, Potential Biochemical Markers for Preterm Labour: A Pilot Study in North India.Indian J Clin Biochem.. 2011 26(1):41-45. [Google Scholar]
[16]. CK Saha, V Jain, I Gupta, N Varma, Serum ferritin level as a marker of preterm labour.Int J Gynaecol Obstet. 2000 71(2):107-11. [Google Scholar]
[17]. LF Gonçalves, T Chaiworapongsa, R Romero, Intrauterine infection and prematurityMent Retard Dev Disabil Res Rev 2002 8(1):3-13. [Google Scholar]
[18]. S Brailsford, J Lunec, P Winyard, DR Blake, A possible role for ferritin during inflammationFree Radic Res Commun 1985 1(2):101-09. [Google Scholar]
[19]. E Gopal, HV Ulmer, RD Nath, Premature labour contractions and the value of serum ferritin during pregnancyGynecol Obstet Invest 1988 26(4):1356-59. [Google Scholar]
[20]. JC Dale, MF Burritt, AR Zinsmeister, Diurnal variation of serum iron, ironbinding capacity, transferrin saturation, and ferritin levelsAm J Clin Pathol. 2002 117(45):802-08. [Google Scholar]
[21]. RF Ritchie, GE Palomaki, LM Neveux, O Navolotskaia, TB Ledue, WY Craig, Reference distributions for the negative acute-phase serum proteins, albumin, transferrin, and transthyretin: a practical, simple and clinically relevant approach in a large cohort.J Clin Lab Anal. 1999 13(6):273-79. [Google Scholar]
[22]. A Siddika, B Nasrin, S Shamim, N Begum, N Nahar, SR Begum, Bangladesh J Obstet Gynaecol. 2009 24(1):14-17. [Google Scholar]