We report cases of ectopic ureter accompanied by three types of ureteral duplication that had been diagnosed previously and treated for enuresis. Data from three female patients ranging in age from 1 to 10 years were evaluated. The ectopic ureter was observed on the left in one case, on the right in another and bilateral in the third case. Complete duplication was found in two cases, while the third had incomplete duplication. Ureteroneocystostomy was performed in one case and subtotal nephrectomy was carried out in the other two cases. Ureteroneocystostomy was performed for the ectopic ureter found in the opposite urinary system in one of the cases. Ectopic duplicated ureter should be considered in treatment-resistant enuresis and urinary tract infections and after a careful physical examination, imaging as well as function tests should be performed.
Enuresis, Ureteral anomaly, Ureteroneocystostomy
Introduction
Duplicated collecting urinary system is the most common anomaly of the urinary system and can be accompanied by complete or incomplete duplication as well as ectopic insertion to all parts of the lower urinary system starting from the distal to the bladder [1–4]. It is usually observed in younger females accompanied by complete ureteral duplication. Most patients are diagnosed by observation of vesicoureteral reflux or dilated ureter [1,2]. However, diagnosis can be difficult in the absence of reflux and dilation and when the kidney pole attached to the ectopic ureter undergoes atrophy. In females with ectopic ureter, specific incontinence in the form of continuous wetness is observed along with normal urinary function. However, this is difficult to diagnose as it is not considered incontinence before toilet training. Nevertheless, it is difficult to make a diagnosis when ectopic ureter is not considered [3].
Here, we present three cases with ectopic ureter diagnosis tested and treated within last one year in our clinic.
Cases
Case 1
The patient was tested and treated for recurring urinary tract infections after birth in our paediatric policlinic. Urinary system ultrasonography revealed no pathology other than slight dilation in pelvicalyceal structures. On the other hand, voiding cystourethrography showed grade 3 and grade 4 reflux on the left and right sides, respectively [Table/Fig-1]. Renal focal defects were found in static renal scintigraphy of the patient who was begun on prophylactic antibiotics. Despite the prophylaxis, urinary tract infection with fever recurred. The patient’s urine was not sterile at the 5-month follow-up. Considering the advanced reflux and renal damage as well as the socioeconomic status of the case, open surgery was planned. During the operation, a third and relatively thin ectopic ureter orifice was found in the cranial site of the left ureteral orifice. After being released and proceeding about 4 cm, this ureter merged with the left ureter [Table/Fig-2].
Voiding urethrocystography: bilateral grade IV vesicoureteral reflux

Distally inserted duplicated ureter observed during ureteroneocystostomy

After excision of this ectopic ureter and repair of the defect on the left ureter wall, bilateral classical Cohen ureteroneocystostomy was performed. Pathological analysis of the excised material revealed a lumen-like structure lined with epithelium. The patient experienced no urinary tract infection during the 1-year postoperative follow-up period.
Case 2
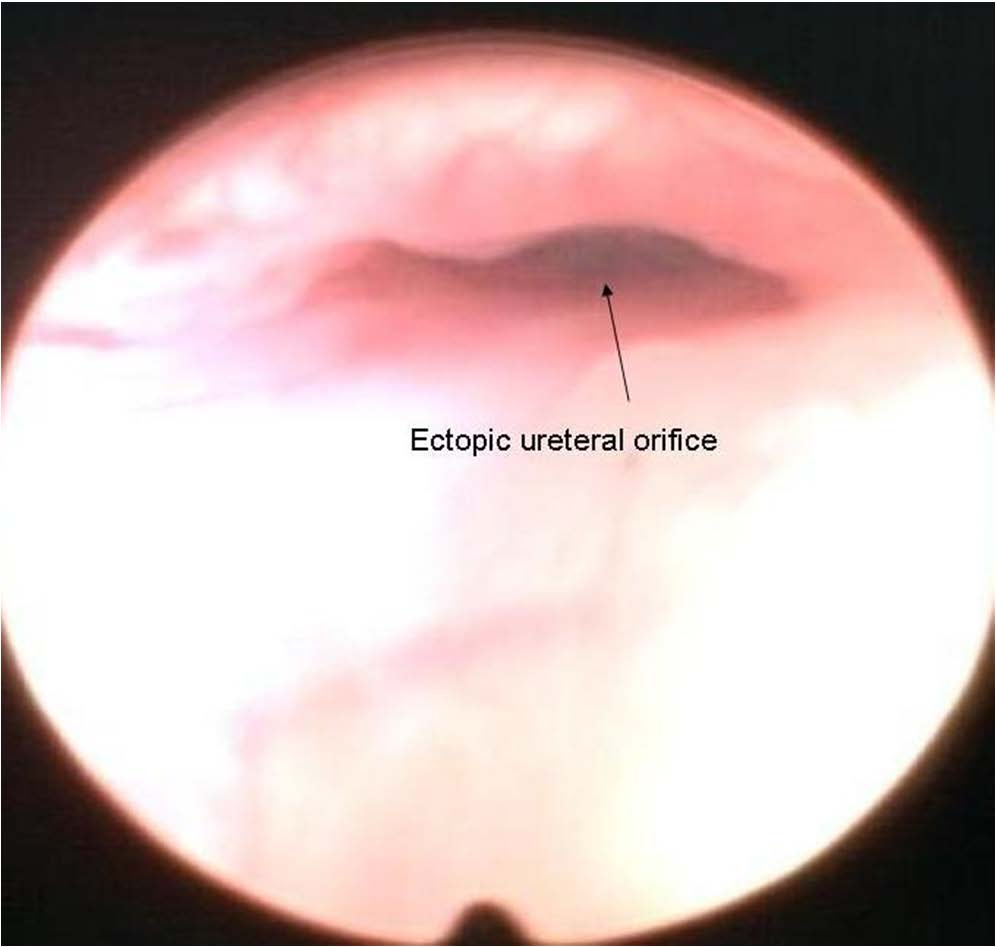
A nine-year-old female patient had been treated for two years due to enuresis and frequent urinary tract infections at another health institution. She had previously undergone urinary ultrasonography (USG), voiding cystourethrography, and intravenous pyelography (IVP) [Table/Fig-3]. Diagnostic cystoscopy revealed a wide-mouthed ureteral orifice that inserted into the bladder neck on the right side [Table/Fig-4].
IVP: no activity was observed in the upper pole of the right kidney

Ectopic ureter orifice in cystoscopic imaging

Static renal scintigraphy showed that the right kidney made a 46% contribution to total function. No tracer uptake was observed in the upper right pole. When the right kidney function was classified within itself, the contributions of the lower and upper poles were 96% and 4%, respectively. Preoperative magnetic resonance (MR) urography was performed [Table/Fig-5]. A double collecting system was observed in the right kidney, which was dilated along with the ureter draining the right kidney upper pole collecting system and inserted into the posterior urethra. Right heminephrectomy was performed. The patient had no postoperative incontinence and no urinary tract infection.
MR urography: dilated upper pole ureter and ectopic insertion

Case 3
A 10-year-old female patient underwent examinations and treatment for five years with a diagnosis of enuresis. She had previously undergone urinary USG five times, renal scintigraphy twice and pelvic computed tomography (CT) once and a diagnosis of left ureter duplication was made. She was treated with oxybutynin hydrochloride. IVP performed after admission to our clinic showed a double collecting system on the right. In addition, a nonfunctional upper pole was detected [Table/Fig-6].
Double collecting system on the right

Urinary USG revealed that the right renal position and pelvicalyceal structure were natural, the left duplicated ureter was dilated, the left upper pole was atrophic and ureterocele was observed in the bladder base. Cystoscopy showed that the ureteral orifice inserted into the posterior urethra [Table/Fig-7]. MR urography was performed and a bilateral double collection system was observed in which the upper left pole ureter was dilated and inserted into the bladder neck. The site of drainage of the right upper pole was not detected [Table/Fig-8]. Left laparoscopic heminephrectomy was performed. As postoperative incontinence was observed, the orifice draining the right upper pole was investigated. The ureter draining the right upper pole was found to be inserted ectopically into the labium minus. As the upper right pole of the kidney was functionally active, ureteroneocystostomy was planned.
Cystoscopic appearance of an ectopically inserted orifice
MR urography: bilateral duplicated ureter and right kidney with dilated nonfunctional upper pole

Discussion
Ectopic ureter is six-fold more common in females than in males, and is generally accompanied by a double collecting system. In 80% of patients, ectopic insertion is observed in the ureter draining the upper pole. The sites of insertion are the bladder neck/urethra (35%), vestibulum (30%), vagina (25%) or uterus (5%) in females, and the bladder neck and prostatic urethra (48%), ejaculatory ducts (8%), and vas deferens (3%) in males [3,5].
Dysplasia occurs in kidney tissue drained by ectopic ureters due to insufficient stimulation of metanephric blastema in the embryonic stage. Examinations in many patients show non functional kidney development. In addition, ureterocele is also common in these patients. Ectopic ureter is a congenital condition, but diagnosis can be delayed until old age in some patients. As the common complaint is incontinence, which is considered a disease of old age, the diagnosis can be delayed. These patients can receive anticholinergic treatment for several years. In addition, in examinations carried out for incontinence, ectopic ureters can be missed while focusing on duplicated ureters. Recurring urinary tract infections are common symptoms in addition to incontinence. Especially if the site of ectopic insertion is distal to sphincter, characteristic incontinence in this condition in the form of continued wetness after toilet training remains. Pain due to dilation can sometimes be experienced because of narrowing in the orifice of ectopic insertion [5]. As nonfunctional kidney tissue is not observed by IVP and renal scintigraphy and the patients concentrate on complaints related to continence, these patients are followed-up for prolonged durations with drug treatment. In general, urinary tract USG is the method of choice for urinary complaints due to its noninvasive nature, ease of performance, and rapidity. USG can generally reveal enlarged ureter traces as well as nonfunctional dysplastic kidney. However, opacity problems are sometimes encountered; these are caused by insufficient urine due to the atrophic upper pole and reduced function. Nonfunctional kidney tissue is not enhanced with contrast material and the dilated ureter is not filled in IVP. In repeated films, an ectopic duplicated system will not be observed, and as the other non-ectopic system is opacified, attention will be focused on that area [6].
If the site of ectopic insertion is outside the bladder in voiding cystourethrography, there will be no opacity in the ureter even in the presence of reflux. In our experience ectopic ureters reflux can reflux on the voiding phase of a voiding cystourethrography. In addition, with use of a Foley urethral catheter in imaging, the ectopic orifice could be blocked by the balloon. Urinary system CT can result in misdiagnosis of ectopic ureter. As the kidney tissue drained by the ectopic ureter is nonfunctional, opacity will not be observed in this area during the examination. Although prolonged exposure improves diagnosis to some degree, the exposure of children to radiation is an important disadvantage [5,6]. However, in MR urography where urine is used as contrast material, as the dysplastic kidney located within the ectopic ureter produces some urine, both dysplastic kidney and dilated ectopically drained ureter can be clearly visualized. However, difficulty of imaging due to claustrophobia and high noise disturbance experienced in MR urography, which necessitate sedation in younger children, are major disadvantages of this method [6].
In the treatment of patients with ectopic ureter, the decision should be based on the functions of the kidney it drains. If the kidney drained by the ectopic ureter is nonfunctional and dilated tortuosity is observed in the ectopic ureter, partial nephrourectomy should be performed. On the other hand, if the kidney drained by the ectopic ureter is functional, ureteroneocystostomy should be performed. In addition to conventional open surgery, the operation can be performed successfully using the less invasive laparoscopic or retroperitoneoscopic surgery technique [7–9]. After the operation, incontinence related to an ectopic ureter should be resolved. Of the cases presented here, the one-year-old with subtotal duplicated ectopic insertion had no urinary tract infection during the 2-year follow-up period after surgery. Similarly, the patient with total duplication and ectopic insertion had no incontinence problems in the 1-year postoperative follow-up period.
Conclusion
In conclusion, ectopic ureter should be considered in cases of continuous incontinence and recurring urinary tract infections. The success rate of the planned examinations will be improved with this pre-diagnosis and use of unnecessary examinations and treatments will be eliminated.
Declaretion: This report was presented at “PEDURO 2014, Antalya – Turkey” as poster session.
[1]. Hanson GR, Gatti JM, Gittes GK, Murphy JP, Diagnosis of ectopic ureter as cause of urinary incontinenceJ Paediatr Urol 2007 3(1):53-57. [Google Scholar]
[2]. Mandell J, Bauer SB, Colodny AH, Lebowitz RL, Retik AB, Ureteral ectopia in infants and childrenJ Urol 1981 126(2):219-22. [Google Scholar]
[3]. El-Ghar MA, El-Diasty T, Ectopic insertion of the ureter into the seminal vesicleWorld J Radiol 2013 5(9):349-51. [Google Scholar]
[4]. Handler TF, Shapiro E, Incontinence in a child with a duplex kidney: case reportRev Urol 2002 4(1):44-48. [Google Scholar]
[5]. Fernbach SK, Feinstein KA, Spencer K, Lindstrom CA, Ureteral duplication and its complicationsRadiographics 1997 17:109-17. [Google Scholar]
[6]. Toprak U, Erdogan A, Pasaoglu E, Karademir MA, The importance of pyelography phase computed tomography in the diagnosis of ectopic vaginal ureterJ Ankara Universty Faculty of Medicine 2007 60(1):35-37. [Google Scholar]
[7]. Plaire JC, Pope JC 4th, Kropp BP, Adams MC, Keating MA, Rink RC, Management of ectopic ureters: experience with the upper tract approachJ Urol 1997 158(3 Pt 2):1245-7. [Google Scholar]
[8]. Tanrıverdi I, Ulman I, Avanoglu A, Endoscopik nephroureterectomy and upper pole nephroureterectomy experience using intra or retro peritonealJ Turkish Association of Paediatric Surgeons 2007 21(1):59-61. [Google Scholar]
[9]. Oge O, Ozeren B, Sonmez F, Nephron-sparing surgery in a duplex system associated with a vaginal ectopic ureterPaediatr Nephrol 2001 16:1135-36. [Google Scholar]