Perforated Gastric Gangrene without Pneumothorax in an Adult Bochdalek Hernia due to Volvulus
John Mathew Manipadam1, George Mathew Sebastian2, Venugopal Ambady3, Ramesh Hariharan4
1 Specialist, Department of G.I. Surgery, Lakeshore Hospital and Research Centre, Maradu, Nettoor PO, Kochi, India.
2 Resident, Department of G.I. Surgery, Lakeshore Hospital and Research Centre, Maradu, Nettoor PO, Kochi, India.
3 Senior Consultant, Department of G.I. Surgery, Lakeshore Hospital and Research Centre, Maradu, Nettoor PO, Kochi, India.
4 Professor and Head, Department of G.I. Surgery, Lakeshore Hospital and Research Centre, Maradu, Nettoor PO, Kochi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. John Mathew Manipadam, Specialist, Department of G.I. Surgery, Lakeshore Hospital and Research Centre, NH-47 Bypass, Maradu, Nettoor PO, Kochi-682040, India.
E-mail: jm_manipadam@yahoo.com
Bochdalek hernia is the most frequent congenital diaphragmatic hernia which occurs due to a defect in the posterior attachment of the diaphragm when there is a failure of closure of the pleuroperitoneal membrane in utero. It rarely presents for the first time in adults. We report one such case of a 23-year-old male patient who presented with an acute abdomen. Chest X-ray showed air under diaphragm and he was taken up for an emergency laparotomy. Intraoperatively an organoaxial volvulus of the stomach was found in a bochdaleks hernia with a focal gangrene of the stomach fundus with perforation and peritonitis. However, there was no breach of pleural cavity. A sleeve resection of the gangrenous portion of the stomach was performed and the diaphragmatic defect was repaired. Patient made an uneventful postoperative recovery. Gastric gangrene with perforation as a manifestation of the adult bochdalek hernia is indeed rare. A concomitant pneumothorax occurs along with this condition which requires an intercostal drainage tube prior to the laparotomy. We report this case for its unique presentation without pneumothorax.
Duodenal ulcer perforation, Laparotomy, Organoaxial volvulus
Case Report
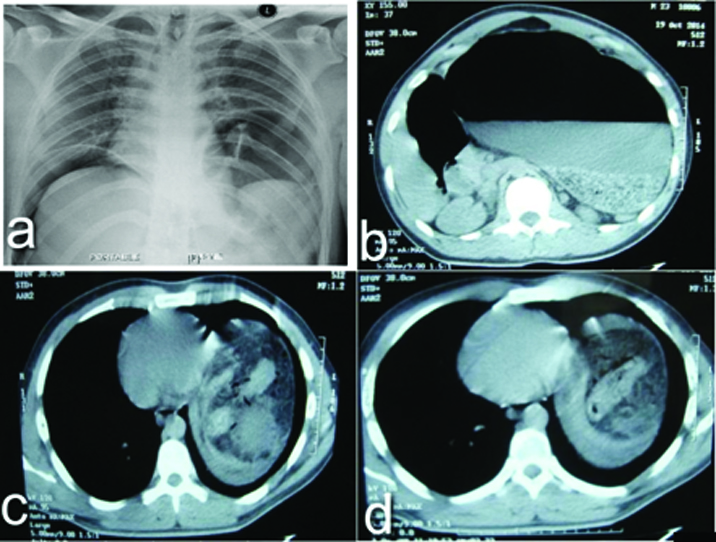
A 23-year-old male patient presented with abdominal pain and vomiting for two days duration. The pain was progressively increasing in severity and generalized to all quadrants of the abdomen over 24 hours. Vomiting was non bilious and contained food particles. He was initially evaluated at a local hospital where Intravenous fluids were given, ryles tube was inserted which had a haemorrhagic aspirate and a Contrast Enhanced Computed Tomography (CECT) of the abdomen was done and the patient was referred to our centre. At presentation, patient had a pulse rate of 140/min, Blood pressure of 100/60, Respiratory rate of 28/ min. Per abdominal examination revealed board like rigidity with obliteration of liver dullness. Patient was resuscitated with intravenous fluids and oxygen by mask. All the lab parameters were sent. Chest X ray erect view showed air under the diaphragm bilaterally with an elevation of the left lobe of the diaphragm compared to the right [Table/Fig-1a]. CECT abdomen done outside was reported as gross distension of the stomach and air within the mesenteric vessels and portal venous system suspicious of bowel infarction [Table/Fig-1b-d]. Leukocyte count was 12,200cells/cumm, serum creatinine - 2.6mg/dl, serum bilirubin - 1.4mg/dl, with haemoglobin of 16.6g/dl.
(a) Chest X-Ray showing air under diaphragm on the right side and herniation of the stomach into the chest on the left side (b-d) CECT abdomen showing air in the mesentery in the herniated portion with gastric outlet obstruction.
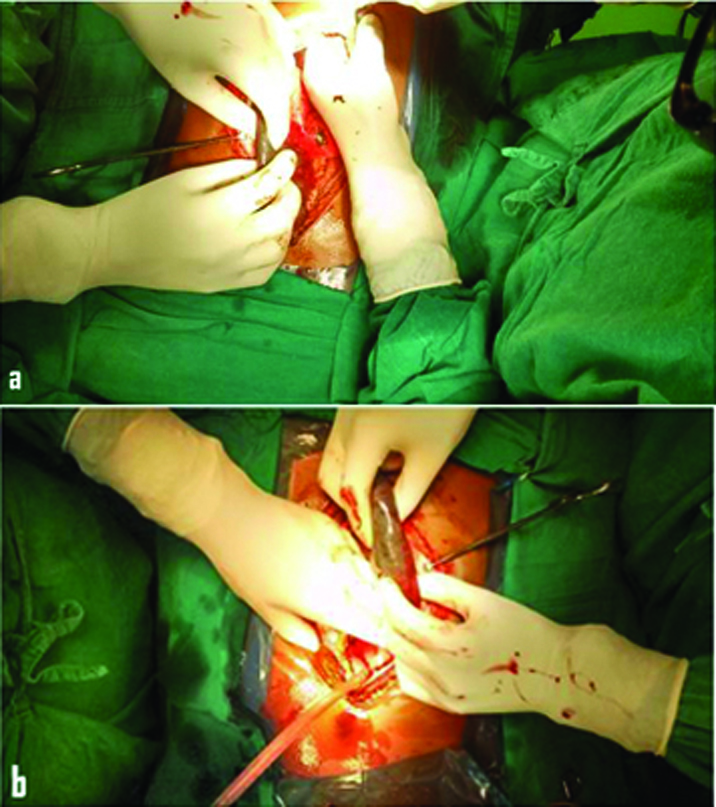
Patient was posted for an emergency laparotomy and proceeded with a provisional diagnosis of duodenal ulcer perforation with outlet obstruction. On entering the peritoneal cavity, there was a transient fire due to ignition of the free gas in the peritoneal cavity by the electrocautery. Intraoperatively to our surprise we found an organoaxial volvulus of the stomach in a bochdaleks hernia with a focal gangrene of the stomach fundus and greater curvature; 5x6 cm in size with a central perforation, with peritonitis [Table/Fig-2a&b]. The spleen and splenic flexure had also herniated into the chest through the defect. However, there was no breach of pleural cavity. We performed a sleeve resection of the stomach to excise the gangrenous portion of the stomach using linear tristapler. The spleen and splenic flexure was repositioned in the abdominal cavity. Repair of the diaphragmatic defect 10x8 cm was performed with interrupted prolene sutures approximating the diaphragmatic muscle edge to the posterior intercostal muscles. Peritoneal toileting and drains were placed prior to closure. Patient made an uneventful postoperative recovery, was started on an oral diet and was stable at the time of discharge.
Showing gangrenous portion of the fundus and greater curvature of the dilated stomach.
Discussion
Bochdalek hernia rarely presents for the first time in adults [1,2]. Such a patient presenting with peritonitis secondary to focal gangrene of the stomach secondary to volvulus is even rarer [3,4]. Volvulus is unlikely in a normal stomach because it is well suspended by gastric ligaments which include the gastrohepatic, gastrocolic, gastrosplenic and gastrophrenic ligaments. However, laxity or absence of these ligaments, diaphragmatic hernias of paraesophageal, traumatic and congenital types; and eventration of the diaphragm all contribute to gastric volvulus [5]. About 100 cases of adult bochdalek hernia had been reported in literature till 1994 [3]. In adults, though majority remains asymptomatic, diagnosis is arrived at when severe complications occur. Even sudden death attributed to adult bochdalek hernia has been reported in literature [6,7]. Stomach is indeed frequently incarcerated in adult bochdalek hernias, however gastric gangrene usually complicates traumatic and paraesophageal hernias [4]. Gastric gangrene with perforation as a manifestation of the adult bochdalek hernia has been reported only thrice before in literature [3,4,8]. It is worth mentioning that in all three of these rarest presentations, the patient also had a concomitant pnuemothorax with mediastinal shift which required an intercostal drainage tube prior to the laparotomy. In the second case even the curative emergency operation was a thoracotomy rather than a laparotomy. In our case scenario the patient did not manifest with pneumothorax probably because the parietal pleura overlying the bochdalek defect remained intact even with the gangrenous volvulus and perforation of the stomach. We report this case for the rarity of its occurrence and for its unique presentation without pneumothorax which required only a laparotomy for its curative treatment unlike the other three cases reported in literature.
Conclusion
Gastric volvulus with gangrene and perforation should be suspected in adult bochdalek hernias presenting with acute abdomen even if there is no pneumothorax on the chest X-ray.
[1]. Bujanda LMD, Larrucea I, Ramos FMD, Munoz CMD, Sanchez A, Fernandez I, Bochdalek’s Hernia in AdultsJ Clin Gastroenterol 2001 32(2):155-57. [Google Scholar]
[2]. Prieto Nieto I, Perez Robledo JP, Hardisson D, Granado de la Fuente A, Bochdalek hernia in an adultScand Cardiovasc J SCJ 1998 32(2):113-14. [Google Scholar]
[3]. Karanikas ID, Dendrinos SS, Liakakos TD, Koufopoulos IP, Complications of congenital posterolateral diaphragmatic hernia in the adult. Report of two cases and literature reviewJ Cardiovasc Surg (Torino) 1994 35(6):555-58. [Google Scholar]
[4]. Ghanem AN, Chankun TSL, Brooks PL, Total gastric gangrene complicating adult Bochdalek herniaBr J Surg 1987 74(9):779 [Google Scholar]
[5]. Shivanand G, Seema S, Srivastava DN, Pande GK, Sahni P, Prasad R, Gastric volvulus: Acute and chronic presentationClin Imaging 2003 27(4):265-68. [Google Scholar]
[6]. Chui PP, Tan CT, Sudden death due to incarcerated Bochdalek hernia in an adultAnn Acad Med Singapore 1993 22(1):57-60. [Google Scholar]
[7]. DeAlwis K, Mitsunaga EM, Sudden death due to nontraumatic diaphragmatic hernia in an adultAm J Forensic Med Pathol 2009 30(4):366-68. [Google Scholar]
[8]. Tuladhar SM, Sharma VK, Delayed presentation of diaphragmatic hernia in a young and fit patient requiring emergency managementJournal of College of Medical Sciences- Nepal 2010 6(3):50-51. [Google Scholar]