To establish the efficacy of definitive fixation using Limb Reconstruction System.
Materials and Methods
Out of 412 compound tibia fractures, 54 cases having Modified Gustilo Anderson Type IIIA and IIIB [6] were included in this prospective study. The study was conducted from 1st June 2013 to 31st August 2015 at KLE’S Dr. Prabhakar Kore Hospital and Medical Research Centre, Belagavi after obtaining the necessary ethical clearance. These 54 patients have undergone fixation using LRS to achieve bony union. Both male and female patients between the age of 18-60 years were included in the study.
Patients with immediate life threatening conditions, closed fractures, osteoporotic fractures and Modified Gustilo Anderson Type I, II and IIIC were excluded from the study.
Intervention
After primary survey and ruling out immediate life threatening conditions, patients were administered intravenous antibiotics and tetanus immunoglobulin. Preoperative work up included complete haemogram, renal profile, coagulation profile, viral markers and radiographs of the affected limbs in orthogonal planes.
Under spinal anaesthesia and with tourniquet in situ, thorough debridement of wound was performed which was followed by LRS application. Stab incisions were followed by blunt dissection until the bone was reached. Shanz pins were passed proximal and distal to fracture site followed by insertion of rail rods and clamps.
In simple fractures without bone loss, LRS was applied in acute docking mode and immediate weight bearing was advised. In those with bone loss, compression distraction technique was used at 1mm for every week alternatively in immediate postoperative period. Patients and their relatives were explained and taught about the technique of compression distraction at a cyclical rate of 1mm per day or on alternate basis. When required, skin grafting and flap surgeries were carried out within 3-4 weeks. Patients were asked to come for follow-up at every 4 weeks interval and weekly dressings were advised to prevent pin tract infection. Clinical and radiological assessment was done at every follow-up to check for pin tract infection and presence of callus. Bony and functional assessment was done by Association for the Study and Application of the Methods of Illizarov (ASAMI) criteria [7].
Results
In this study, LRS was performed in 54 cases of open fracture tibia (type IIIA and type IIIB). The patients were between 18-60 years of age with a mean age of 42± 5years. A total of 49 patients were male and 5 patients were female and road traffic accident being the most common cause of injury. Forty patients had fractures in middle one-third tibia shaft. Acute docking was done in 47 patients [Table/Fig-1,2,3,4,5 and 6] and 1 patient underwent LRS fixation for bilateral tibia fractures [Table/Fig-7,8 and 9], 7 patients with bone loss underwent bone transport [Table/Fig-10,11] and 8 patients underwent split thickness skin grafting and flap repair. One patient with type IIIB fracture developed deep infection with pin loosening which warranted fixator removal, it was reapplied after the infection was under control. In 3 patients with type IIIA fracture, fibular osteotomy was done [Table/Fig-9,10], as intact fibula was not allowing compression at the fracture site. The most common complication encountered in this study was pin tract infection, which was treated with suitable antibiotics postculture and sensitivity testing. All patients achieved good range of movements in the follow-up period. Among 54 patients, bony results as per ASAMI score were excellent in 67% (n = 36), good in 25% (n = 14), fair in 4% (n = 2) and poor in 4% (n = 2). Functional results were excellent in 80% (n = 43), good in 13% (n = 7), fair in 7% (n = 4) [Table/Fig-12]. All the 54 cases of type IIIA and IIIB were kept on LRS external fixator for a period of 5-6 months on an average depending on the rate of union, after which the fixator was removed and limb immobilized with Patella Tendon Bearing cast for another 3-4 weeks. In most cases union was complete by 7-8 months, the least being 5 months for a tibia shaft fracture. In cases with acute docking [Table/Fig-13], patient satisfaction post-surgery was excellent because fixation allowed them to start immediate weight bearing. Patient satisfaction was assessed using a questionnaire wherein majority of patients expressed high satisfaction in terms of early mobilization. The average hospital stay for the patients was 7 days and as compared to multi staged surgery financial burden was reduced by 40%. The average time of return to work for the patients was 20 days.
Showing open distal tibia fracture; Showing open distal tibia fracture.

X-ray showing distal tibia and fibula fracture AP view.


Post op X-ray AP and lateral view showing LRS in situ.

Follow up X-ray AP view with LRS in situ.

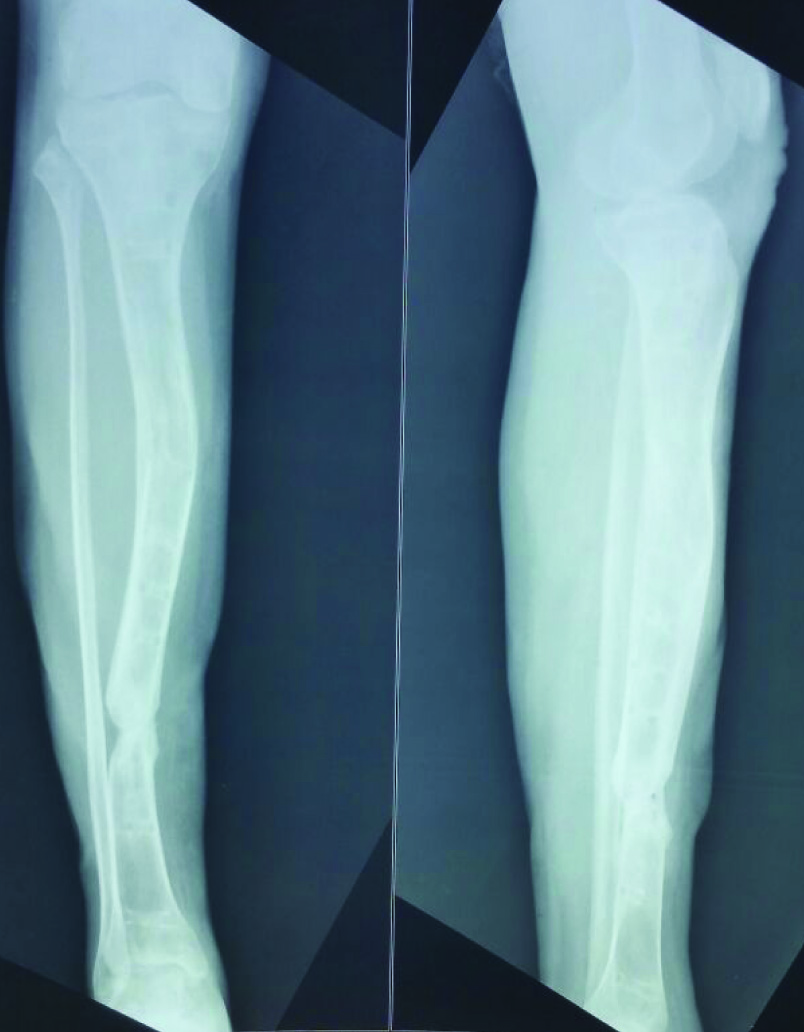
Showing X-ray AP and lateral view after LRS removal with good union.

LRS applied to bilateral lower limbs.

X-ray AP and lateral view right leg.

X-ray AP and lateral view left leg.

Xray showing bone transport.

Xray showing AP and Lateral views post bone transport.
Bony and Functional results as per ASAMI criteria.
| Bony Results | | Number of patients |
|---|
| Excellent | Union, no infection, deformity<70, limb length discrepancy <2.5 cms | 36 |
| Good | Union + any two of the following: No infection, deformity<70, limb length discrepancy <2.5 cms | 14 |
| Fair | Union + any one of the following: No infection, deformity<70, limb length discrepancy <2.5 cms | 2 |
| Poor | Nonunion/refracture/union+infection+deformity>70 + limb length discrepancy > 2.5 cm | 2 |
| Functional Results |
| Excellent | Active, no limp, minimum stiffness (loss of <15 knee extension/< 15 dorsiflexion of the ankle), no reflex sympathetic dystrophy, insignificant pain | 43 |
| Good | Active with one or two of the following: Limp, stiffness, RSD, significant pain | 7 |
| Fair | Active with three or all of the following: Limp, stiffness, RSD, Significant pain | 4 |
| Poor | Inactive (unemployment or inability to return to daily activities because of injury) | 0 |
| Failure | Amputation | 0 |
Results of open tibia fractures fixed using LRS.
| Criteria | Number of patients |
|---|
| Acute Docking Mode | 47 |
| Bone transport | 7 |
| Split thickness skin grafting and flap | 8 |
| Fibular osteotomy | 3 |
| Resuturing | 4 |
| Pin reapplication | 1 |
| Average time of union | 28 weeks |
| Average time of implant removal | 30 weeks |
Discussion
Open fractures of tibia are very common in this modern world because of high velocity road traffic accidents. Although newer and better treatment approaches for the management of open fractures are available, open fractures remain to be one of the important challenges in orthopaedic trauma. Because the study has been done in a tertiary care centre, a lot of compound fractures were encountered. According to Behrens and Searls [8], every year two cases out of 1000 injuries were compound tibial fractures and this rate was even greater than 0.2% in developing countries. The various modalities of treatment available for tibial compound fractures are minimal osteosynthesis, biological fixation and internal fixation with intramedullary nailing or external fixation with different types of fixators. Irrespective of which treatment method is used, the aim of the surgery should be to obtain maximum functionality to the fractured extremity and to maintain patient’s life quality with minimum damage or complication [9–11].
Use of external fixators in comminuted, defective, and contaminated open fractures like Gustilo-Anderson types IIIB and IIIC open fractures, is routinely accepted these days [12,13]. According to Yokoyama K, treatment of grade IIIB and IIIC with intramedullary nailing was risky as it lead to deep infection and nonunion in 20.3% cases [14]. Therefore, external fixators are preferred modality because they are easy to use and allow soft tissue treatment. But the problems associated are prolonged immobilization and need for revision surgery for definitive fixation at a later stage. Therefore, LRS, which is different from the simple external fixators in allowing full weight bearing immediate postoperatively like an intramedullary fixation was used. LRS fixation technique also has an added advantage of salvaging the limb and preventing amputation. On other side, it has its own complications like pin loosening and pin tract infection. In this case series of 54 cases, pin loosening was noted and pin replacement was required only in 1.85% cases and moreover, in 92.59% cases, complete union was achieved within 8 months.
The complications of nailing or fixators with acute docking are shortening, soft tissue healing problems, increased morbidity, multiple surgeries, prolonged hospital stay and its consequences like deep vein thrombosis, bed sores, nosocomial infection which eventually leads to increased chances of mal union and non-union and increased financial burden [15]. In a study conducted by Edward in 1988, Grade III open tibial fractures were treated with external fixator, where in 93% of the fractures united well and 89% patients had satisfactory clinical function [16]. Even in patients treated with secondary nailing after primary external fixator or after delayed primary nailing there are more chances of infection [4]. Illizarov ring fixator is a good modality of treatment but is cumbersome for the patient and difficult to master by the surgeon as compared to LRS. According to a study done by Ajmera et al., LRS proved to be an effective modality of treatment in cases of open fractures tibia with bone loss as definite modality of treatment for damage control as well as for achieving union and lengthening [17].
LRS fixator provides immediate stability to fracture fragments and allows immediate weight bearing which ultimately promotes early fracture healing and reduced financial burden.
Limitation
Limitations of this study were a lack of comparison group or a control group and less sample size. Considering the optimistic results of the study, further multicentric studies and randomized control trials are suggested before establishing it as an effective modality of treatment in cases of open fractures tibia with bone loss.
Conclusion
LRS is a simple and easy system which can be used for all open fractures. Fixation with LRS is a single definitive surgery. It is a cost-effective mode of treatment. Patient is independent and walks full weight bearing without walking aids. It saves time for the patient by reducing hospital stay and is a simple technique compared to Illizarov ring fixator. Patient compliance is excellent. It can also be used for bone lengthening / transportation, deformity correction, in patients with infective non-union and osteomyelitis. Implant can be reused which brings down the cost of surgery considerably.