So, the depth of assimilation of these guidelines among common population or a specific special group needs to be assessed [10]. Earlier researches have noted substantial improvement in hand hygiene behaviour among school children in various study settings [11]. But all the studies resulted in a subjective inference with lack of objective comparability and quantification.
It is the school where a drive has to be created to optimise hand hygiene practices. Can it be alcohol based hand rub or soap and water based hand hygiene maintenance technique, step by step follow-up of the guidelines are very necessary to involve all the surfaces of our hand [12–14].
Improvement of hand hygiene with the aim of minimizing infections and communicable diseases is at the high priority of WHO [15]. Children are primary victims of communicable diseases especially in developing regions globally [15]. Despite all these noticeable progress there still persist catastrophic lacunae, that many a times goes unnoticed. According to UNICEF (United Nation International Children’s Emergency Fund), hand washing with soap is not a widespread practice in India [16,17].
Gender inequality along with specially abled group of population is a vulnerable group of population that have to be given extra care in every context of public health. Poor hand hygiene plays a significant role in faecal-oral route of transmission of disease. Diarrhoea and respiratory infections are the primary cause for child deaths in India leading to more than 1,000 child deaths due to diarrhoea alone per day [17]. The Government of India has improvised and institutionalised hand washing with soap in school before mid day meal amongst 110 million children in 1.4 million schools, but efficient applicability and accountability is still at stake [17,18]. According to previous studies, it has been noted that diarrhoea and respiratory infection are leading cause of deaths in India [19].
India being a developing country, one of the rapidly emerging economies globally and with the second largest population and taking rest of the said factors under consideration, is the ideal location to conduct the study [20,21]. Hence, the present study was designed to assess effectiveness of hand hygiene using Graphical Assessment Technique (GAT) among specially abled and government school children of Delhi, India.
Materials and Methods
Setting: Two institutions namely National Association of Blind School, R. K. Puram, New Delhi, India and a government school within a mile radius, were considered for the study just to satisfy the comparative need. Both the institutions are co-educational and cater education to a wide sector of society. Permission for the study was obtained from both the institutions before the commencement of the study. The schools cover educational needs of students from adjoining states of north India. National Association of Blind School, New Delhi, India, is a foremost educational institution that provides all-round academic and life supportive skills to specially abled children especially the blind children and those with multi organ disorders. The institution stresses and pays individual attention to every child to excel in life like every other normal individual. The school conducts preparatory classes for the newly admitted students so that they adapt and improve their psycho-motor abilities. The National Association of Blind School, New Delhi, India, presently caters education to around 300 students, of which majority stay in-house. The other school selected was a government school with total strength of around 2000 students.
Reliability and Validity: This study can be used to check the feasibility and relevance of the technique. It was also tried to check if visual acuity has any effect on hand scrub motion.
Training and Calibration: A day of training session was carried out for standardization and calibration for the monitoring of hand hygiene practice and follow-up was carried out at the National Association of Blind School for a group of four teachers and two instructors. The training session consisted of a revaluation of the WHO hand hygiene guideline, followed by re-demonstration by each of the teachers and instructors [15].
The internal reliability for the examiners were assured using Cronbach’s alpha coefficient (0.85). Ethical approval was obtained from institutional review board of Divya Jyoti College of Dental Sciences and Research, Modinagar, Ghaziabab, Uttar Predesh, India. Informed consent was individually obtained from every participant/guardian after explaining the study. It was found that proper explanation of the items was necessary to maintain step by step understanding of the concept and prevent misinterpretation, which was done by the principal investigator.
Data Collection: The prime assessment technique used in this study was GAT.
Since, this study was the first and one of its kinds of objective analysis that applies GAT and so was conducted in a pilot study model. An equal strength of 40 students of age 15 years were selected randomly using random sampling lottery method from each school with gender wise equality that is 20 females and 20 males. It was seen to that all the students selected were of similar socio- economic status and similar intelligence quotient level according to the records maintained at the official database by individual schools. Only those students from the blind school who have visual impairment more than 80% were selected and devoid of any multi-organ or psychomotor disorders. NABS students are routinely checked for their overall medical condition and so, it proved to be a valuable resource.
The goal of intervention was to improve hand hygiene with special emphasis on WHO hand hygiene maintenance guidelines and relevance of hand hygiene in day to day life. The students were sensitized regarding the importance of hand-washing and when to wash hands through interactive sessions by teachers and blind school instructors for blind children. Audio-visual demonstration was given to both the blind school and government school children in batches of 10 and was reinforced with tactile demonstration with the help of teachers and instructors in both the institutions. To encourage student participation in the program a speech competition was conducted after emphasising the role of hand-washing in prevention of diseases to positively reinforce the need for hand hygiene maintenance between each intervention. Three interventions were given and four teachers and two instructors were individually taught in both institutions according to step by step guideline published by the WHO [15]. The training was given using an audiovisual aid and using live demonstration given by the principal investigator. The instructors were directed to reinforce the hand hygiene demonstration according to WHO guidelines daily during recess or before the subjects under study had lunch, and the children washed their hands under the supervision of trained instructors for the entire period of the study.
Graphical Assessment Technique (GAT): This is the first novel technique that has been devised and introduced to ascertain the efficacy with which the hand hygiene guidelines are being followed. This arbitrary technique of graphical assessment makes use of ultraviolet sensitive fluorescent gel and powder, ultraviolet lamp, non toxic water based paint and graph sheets for hand hygiene assessment. It was made sure that armamentarium used were non-toxic, non-mutagenic and non-irritant to tissue. The concept of arbitrary GAT is all about analysis of individual mindset on hand hygiene and its application while washing hands since the subjects fail to follow the standard guidelines published by various committed international public health and research organizations either due to ignorance or carelessness.
This technique is not a tool to assess microbial load or efficacy of hand sanitizing agents used. The salient feature of this technique is the evaluation of efficacy with which an individual follows the WHO hand hygiene guidelines because that produces a significant impact on the amount of area of hand wetted and washed during a routine application of soap or alcohol based hand rub. Many a times we overlook multiple areas of hand that have to be cleaned systematically. This study that improvises the graphical assessment or arbitrary technique is first and one of its kind of a tool that allows us to estimate, quantify and compare the efficacy of hand hygiene guidelines follow-up. The technique is salient in the matter of simplicity and flexibility of use in any environment with any efficient hand hygiene guideline. The objective results may be quantified and compared for data maintenance pertaining to hand hygiene prospective evaluation.
Overview of the Arbitrary Graphical Assesment Technique (GAT)
Check how a person usually washes hand and obtain a pre examination idea of the same and note down the time taken. Block visual sensitivity of the subjects under examination after obtaining the informed consent [Table/Fig-1].
Now, apply 1gm of Ultraviolet (UV) sensitive fluorescent gel onto each of the finger tips and middle third of the palm [Table/Fig-2].
Similarly apply same amount of UV fluorescent pink powder on the same portions of the hand.
Ask the subject to proceed with their usual motion of hand washing technique and note time and compare with the time already noted.
Now, if the post and pre-application time correlate continue onto the next step, if not repeat the procedure after washing the hands with soap and water and drying it.
NOTE: Time has to be noted only from the point when the individual commences the demonstration of his/her hand hygiene procedure and is to be stopped when the individual concludes it.
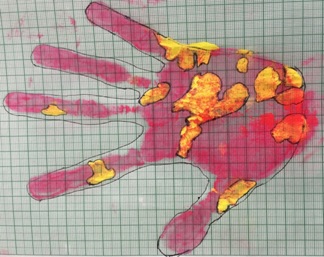
In the dark room using UV lamp delineate the areas covered while the hand hygiene motion [Table/Fig-3] and the areas leftover are marked using a fine end brush and water based non-toxic paint and guided to be placed onto a graph in a steady motion by keeping the fingers spread apart. The outline of the hand is marked with a fine tipped 0.5 mm marker carefully outlining the portions that are in contact with the graph paper [Table/Fig-4]. In the next step, the subject slowly takes off the hand from the paper and the subject is instructed to wash off his/her hands. The graphical analysis was applied on every individual after ultraviolet evaluation by the principal investigator.
NOTE: An overall lesser percentage of area covered with the UV fluorescent gel and powder indicates better hand scrubbing technique.
In the final process percentage of area not covered during hand hygiene maintenance procedure was noted [Table/Fig-5].
Hand wash practiced by the subject.

After the application of ultra voilet flurocent GE.



Assessment outline with markings on graph
Statistical Analysis
The collected data was analyzed using SPSS software (version 20.0); Chicago; IL, USA. The data was subjected to descriptive analysis and parametric tests were used. Paired t-test were used to test the difference between each of the interventions and unpaired t-test to compare between the special group and the comparative group of government school children.
Results
As part of the study the numbers of participants were tabulated from the institutions directory and a total of 40 participants were included from each of the institution summing up to a total of 80 participants. The participants were analyzed for hand hygiene using the GAT and the area not covered or cleaned during the action of hand hygiene was noted in percentage out of the total surface of the hands both dorsally and ventrally. [Table/Fig-6] shows the details of total number of participants with equal distribution of 20 male and 20 female students of 15 years age group.
Demographic data of subjects under study.
| Group | N | Mean |
|---|
| Age (Years) |
| Group 1* | 40 | 100% |
| Group 2# | 40 | 100% |
| Gender |
| Male | 20 | 50% |
| Female | 20 | 50% |
* Group 1- National Association of Blind School, New Delhi, India.
# Group 2- Government School, New Delhi, India.
[Table/Fig-7] explains the mean scores of percentage area uncovered during the hand washing procedure that is the baseline data mean score of 10.08, immediate post-intervention score of 10.06, one week post-intervention score of 9.54 and one month post intervention mean score of 6.87. On applying statistical tests a significant difference between the means score was noticed among the base line mean score of blind children and post- intervention analysis at one week and one month. [Table/Fig-8] explains the mean scores of percentage area uncovered during the hand washing procedure in government school students, that is the baseline data mean score of 11.96, immediate post- intervention score of 11.95, one week post intervention score of 11.96 and one month post-intervention mean score of 10.59. On applying statistical tests a significant difference between the means was noticed among the pre-intervention base line mean score of government school children and only at one month.
Intra group descriptive statistics-group i- NABS students.
| Interventions | Mean % (S.D) | p- value | t- value |
|---|
| Pre-intervention | 10.08(1.91) | 0.105 | 1.657 |
| Immediate post-intervention | 10.06(1.90) |
| Pre-intervention | 10.08(1.91) | 0.001* | 11.782 |
| Post intervention-1 week | 9.54(1.91)* |
| Pre-intervention | 10.08(1.91) | 0.001* | 20.592 |
| Post intervention-1 month | 6.87(1.69) * |
* (p) ≤0.05
Mean percentage group scores-group ii- government school students.
| Interventions | Mean % (S.D) | p- value | t- value |
|---|
| Pre-intervention | 11.96(2.10) | 0.138 | 1.514 |
| Immediate post-intervention | 11.95(2.10) |
| Pre-intervention | 11.96(2.10) | 0.076 | 1.822 |
| Post intervention-1 week | 11.96(2.09) |
| Pre-intervention | 11.96(2.10) | 0.001* | 15.280 |
| Post intervention-1 month | 10.59(2.07)* |
* (p) ≤0.05
Subsequently, a significant difference (p≤0.05) between the study groups was noticed regarding the base line mean scores and subsequent post-intervention evaluations. [Table/Fig-9] explains the significant difference (p<0.01) between the analysis interventional scores of both the groups.
Mean percentage scores difference following intervention between blind and government school children.
| Group I*Mean% (SD) | Group II #Mean% (SD) | t- value | p- value |
|---|
| Pre-intervention | 10.08(1.91) | 11.96(2.10) | -4.179 | 0.001* |
| Immediate post-intervention | 10.08(1.91) | 11.95(2.10) | -4.158 | 0.001* |
| Post intervention-1 week | 9.48(1.90) | 11.95(2.09) | -5.516 | 0.001* |
| Post intervention-1 month | 8.39(2.01) | 10.59(2.07) | -4.820 | 0.001* |
* (p) ≤0.05
* Group 1- National Association of Blind School, New Delhi, India.
# Group 2- Government School, New Delhi, India.
Discussion
The present study utilizing the Graphical Assessment Technique (GAT) is the first technically salient study that objectively analyses and compares the improvement in hand hygiene practices among blind children and government school children. The primary advantage of this tool is its ease of applicability and utilization on any study population. An overall lesser mean percentage score of uncovered area following hand scrubbing indicated better hand hygiene. In the study, analysis between the two groups of school children namely, National Association of Blind School (NABS) children and government school children showed a significant difference on statistical analysis between each of the said interventions like immediate post-intervention, one week post-intervention, one month post-intervention percentage scores and even the pre-intervention baseline evaluation scores. The mean scores were comparatively lower in case of NABS children as compared to government school children signifying a net improvement in hand hygiene practice and follow-up of the blind school children. Lower mean score percentage (10.08±1.91) when compared to government school children (11.96±2.10) could be due to the implementation of basic hygiene course imbibed into the curriculum of the blind school along with training provided by specialised instructors to improve their psychomotor skills and make them competent for their day to day competencies of the world. The NABS, New Delhi also conducts special preparatory classes for those new children who are admitted to the school every academic year along with the Indira Gandhi National Open University, New Delhi, India. But comparatively net lower hygiene practice in government school children might be because they are less pre accustomed to basic lifestyle and hygiene training.
When we look into the individual groups under study, the proportional variation can be noted even in the intra group analysis. On evaluation of the blind children, a noticeable non-significant (p≥0.05) variation in hand hygiene technique and protocol at the baseline (10.08±1.91) and immediately after intervention (10.06±1.90) was noted while a significant difference (p≤0.05) was noted after intervention and when the percentage scores of area of the hand not covered during hand washing was marked at one week (9.54±1.91) and one month (6.87±1.69). On the contrary along with comparatively poor hand hygiene practice of government school children that was noted before the intervention (11.96±2.10) on assessment showed non-significant (p≥0.05) improvement even at the immediate post intervention (11.95±2.10) and at one week analysis (11.96±2.09). This indicates the need for repeated reinforcement of proper hand hygiene technique. But a gradual significant (p≤0.05) improvement was noted at one month analysis (10.59±2.07) from the baseline data. This could be due to improved psychomotor skills, auditory and tactile perception among the blind children since they lack visual acuity and also have improved dependence on rest of the sense organs.
Since this study is first of its kind it cannot be compared with any other similar studies. Recent relevant articles found had focussed on improving and improvising proper and efficient hand hygiene among school children using only questionnaire or assessment of microbial load, with no study reported on objective analysis following WHO hand hygiene technique intervention. There is variation in the range of hand hygiene studies conducted over the past many decades and their changing relevance. The major difference was based on their types of intervention, questionnaire, evaluative studies related to various hand hygiene practices, health education, microbial load, numerous agents used to maintain and improve hand hygiene measures. Our primary aim of study was to throw light on an urgent requisite of an objective evaluation technique to quantify hand hygiene.
Our study along with studies conducted in both developed and developing countries pointed the positive influence of hand washing promotion in reducing the incidence of diarrhoea and respiratory diseases. An analysis conducted in West Bengal by SK Ray et al., India showed; children who lived in household where mothers washed their hands intermittently and specifically after defecation with soap had lesser diarrhoea than children of mothers who did not use soap [22].
It was noted that there is paucity of literature relevant to our present study, since none of the studies objectively evaluated the follow-up or improvement in the hand washing guideline as published by the WHO [15].
It has been noted in multiple studies that unsoiled contaminated hands were effectively cleaned using alcohol based hand rub than antiseptic soap. It was also noted that alcohol based hand rub was superior to standard hand washing technique [22,23]. The program also showed a positive effect on the hand washing practices among the students gradually over a month in government school children and a week in blind school children with significant improvement in routine hand hygiene follow-up by children. Multiple studies in India and abroad have also demonstrated similar improvements in student’s knowledge, attitude and practices with regard to hand-washing.
A baseline study of a large intervention in hand washing behaviour in rural Bangladesh published by Luby SP et al., also found that the respondents who had households with children under the age of 5, usually only rinsed their hands with water at critical times of hand contamination [23]. A study in Karachi, Pakistan, by SP Luby et al., had demonstrated that regular hand washing whenever required and bathing with soap is effective in preventing both diarrhoea and pneumonia [24]. Another study by Ray SK et al., from Kolkata slums indicated that hand washing with soap may reduce the incidence of dysentery cases in the community. Numerous hand hygiene promotion studies have noted an improvement in hand hygiene [25].
Since this is the first study that uses a new tool for objective assessment of hand hygiene, a limited sample of blind children and government school children has been studied along with the testing of the probe on both normal and special population groups. This enables a quantification of percentage proportional scores between every group of population and empowers systematic comparison, as well as review of the protocol of hand hygiene followed around the world. This technique showed development in perception about hand hygiene among both the groups considered for the study implying its applicability even on general population.
Advantages
The GAT can be used to evaluate an individual’s level of hand hygiene maintenance, by not stressing on the type of agent used, as the relevance of physical hand scrub is more when compared to the chemical agent used for the same. Ease of use with limited armamentarium provides this technique reproducibility and simplicity. This technique provides a modality for self motivation and public health school evaluation programmes along with studies pertaining to the epidemiology of infectious diseases and their varied transmission in different population groups. It also opens a new vista of hand scrub evaluative and comparative assessment protocol. Since, the favourable results of this present study pointed onto the applicability of the graphical technique on both special and general population, it shows the flexibility, applicability and its use in comparative analysis.
Limitation
In GAT, inter-digital regions cannot be noted. But it provides a definite link to an individual’s hand hygiene maintenance and practice. Systematic follow-up and calibration between the graphical estimators is the core requisite otherwise might lead onto inconsistencies. Since, other than principal investigator the rest of investigators who maintained the routine hand hygiene reinforcement in both the schools were different, the varied basic inherent capacity of the instructors to teach along with their professional qualification might have caused a lacunae of bias.
Recommendation
Routine hand hygiene assessment as part of annual school health progress report should be made mandatory, taking into consideration its ample advantages of averting infections.
Further longitudinal studies with larger sample size should be carried out to prove its adequacy for studies on epidemiology of infectious diseases due to inadequate hand hygiene.
The graphical assessment technique must also be tried and tested on geriatric population because of their vulnerable sensitivity and susceptibility to infections.
Conclusion
The arbitrary graphical assessment technique is a stepping stone to hand hygiene assessment and follow-up and will empower healthcare organizations to objectively assess, quantify, modify the guidelines according to the needs of varied population and enable comparability for efficient monitoring. The study can help health policy makers in formulation of hand hygiene guidelines. Further, hand hygiene habits can be improved through sustainable monitoring by trained instructors. The relevance of this study can be noted in the fact that it enables stepwise analysis of every population group on hand hygiene. Since, hand contamination is not just a concern while ingesting food but can be a culprit to various infections even in the day to day routine. This pilot study would pave a milestone in hand hygiene comparative analysis and follow-up protocol, though it needs expansive studies that include evaluation of multiple population groups along with modification of the technique at its innate capacity to assess every specially abled population.
* Group 1- National Association of Blind School, New Delhi, India.
# Group 2- Government School, New Delhi, India.
* (p) ≤0.05
* (p) ≤0.05
* (p) ≤0.05
* Group 1- National Association of Blind School, New Delhi, India.
# Group 2- Government School, New Delhi, India.