Dental caries is one of the common infectious disease affecting children and adults worldwide [1,2]. Dental caries develop when there is an imbalance between the commensal organism and cariogenic organisms. Cariogenic bacteria like Streptococcus mutans, Actinomyces species and Lactobacillus produce various acids by the metabolism of carbohydrates and these acids in turn demineralize the enamel surface [3]. This acidic environment causes a drop in pH level below 5.5, resulting in demineralization of hydroxyapatite crystals leading to dental caries. Dental caries is one of the most prevalent and important dental problem affecting most of the children in India [4]. Dietary patterns which include more of carbohydrates and sugars are the predominant cause for the high prevalence of dental caries which affect the primary dentition more than the permanent dentition [5,6]. Karunakaran R et al., [7] conducted a study to evaluate the prevalence of dental caries among school going children in sub-urban area of south India and reported an overall prevalence of 65.9%. The authors highlighted upon the fact that most of the caries lesions were not treated [7]. The most proven and effective method in the prevention of caries is the regular use of fluoride for its cariostatic properties. With the widespread use of water fluoridation, the overall smooth surface caries rate has decreased significantly [8]. The occlusal surfaces of the teeth usually have pits and fissures which provide a good environment for demineralization with minimal salivary access and make them caries prone [9], this could be the reason, occlusal caries account for 56% to 70% of the lesions in children aged 5 to 17 years [10]. The success of pit and fissure sealing materials is highly dependent on the marginal sealing ability of the fissures. If there is a breach in the marginal integrity of the sealing material subsequently leading to bacterial colonization under the restored fissures and thereby initiating and progressing the carious lesion beneath the restoration [11]. There are several commercially available pit and fissure sealants which include Clinpro, Helioseal F, Ultraseal XT, Glass Ionomer Cement (type IV). The more recently introduced and more widely used pit and fissure sealants in clinical practice in India are Clinpro and Helioseal F. There is limited literature evidence on the clinical efficacy in terms of marginal sealing ability of these two sealants. With this background the present study was carried out to evaluate and compare the marginal sealing abilities of Clinpro and Helioseal F pit and fissure sealants.
Materials and Methods
A total of 50 human premolar teeth were used in this invitro study. The study was approved by the Institutional Ethics Committee. The study was conducted from November 2014 to June 2015. Teeth were obtained from patients undergoing extraction for orthodontic reasons only. All the extracted teeth were non hypoplastic and non carious and were divided into two groups. Group 1 included 25 teeth for application of Clinpro sealant and Group 2 included 25 teeth for application of Helioseal F sealant.
Sample Preparation: After extraction, all teeth were cleaned of gross debris, disinfected with hydrogen peroxide solution then were stored in artificial saliva at room temperature. Artificial saliva was prepared following the composition recommendation by Sieck B et al., [12]. All fissures in each tooth were cleaned for 15 seconds with aqueous slurry of 5g pumice/4ml water using a rubber cup in a slow-speed contra-angle hand piece. The teeth were rinsed with air-water spray. Prior to sealant application two coats of varnish was applied on all the teeth surface except for 1mm diameter surrounding sealant and allowed to dry. Teeth in both the groups were etched with 37% phosphoric acid gel for 20 seconds. Then were rinsed with water for 20 seconds and lightly dried with three way syringe. Teeth were visually inspected to demonstrate a uniform frosty appearance.
Steps in placement of Helioseal-F sealant: After etching and drying Helioseal F pit and fissure sealant was applied directly with the disposable cannula. Sharp explorer was used to remove any air bubbles and uniform flow of the material was ensured. After 15 seconds the sealant was cured with a suitable polymerization light for 20 seconds.
Steps in placement of Clinpro sealant: After etching and drying Clinpro pit and fissure sealant was applied directly with the disposable cannula. Sharp explorer was used to remove any air bubbles and uniform flow of the material was ensured following which the sealant was cured with a suitable polymerization light for 20 seconds.
Each tooth was checked with an explorer for complete coverage and retention of the sealant. Samples were stored in artificial saliva for 72 hours before thermocycling.
Thermocycling: Thermocycling was carried out at the Department of Physics, Anna University, Chennai, India. The purpose of thermocycling was to simulate the oral environment. All the teeth in both the groups were subjected to thermocycling at 5oC, 37oC, and 55oC for 500 cycles with a dwell time of 30 seconds and stored in artificial saliva before being tested for microleakage. A glass beaker immersed in a box of ice was used to maintain the temperature at 5oC and another glass beaker placed on hot plate was used to maintain the temperature at 55oC. A thermometer was placed to check the temperature periodically and care was taken to ensure that all the teeth were completely immersed. Immersion time was recorded using a stop watch.
Dye Penetration: The samples were immersed in 2% methylene blue solution for 24 hours. After removal, all the samples were washed in plain water to remove excess dye. The root portions of the samples were removed and then the crown portions were sectioned buccolingually into two halves using a diamond disc and high speed lathe. The sectioned samples were examined under an Optical Stereomicroscope (Carl Zeiss Stereo discovery V8, Germany) at crystal growth center, Anna University, Chennai, India. The extent of dye penetration was evaluated at a magnification of 40 X. The degree of microleakage was scored by a single observer using Williams B and Winter GB criteria for evaluation of dye penetration [13].
Criteria for Grading Microleakage
Grade 0: No dye penetration.
Grade 1: Dye penetration extending one third the total length of the interface between the sealant and tooth structure.
Grade 2: Dye penetration extending between one third and two thirds the total interface length.
Grade 3: Dye penetration extending beyond two thirds of the total interface length.
Statistical Analysis
The results were tabulated and the data were analyzed statistically using statistical package SPSS Version 17. In the present study frequency of degree of microleakage was found out by comparing the dye penetration in both the groups by using Chi square test and Mann Whitney Test. A p-value of less than 0.05 was considered to be statistically significant.
Results
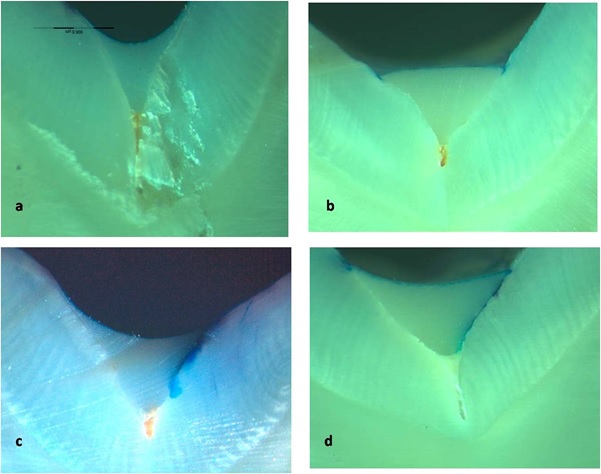
When the two groups (Group I-Clinpro and Group II-Helioseal F) were compared in terms of the extent of microleakage based on the amount of dye penetration between the sealant and tooth substance interface, it was seen that in Group 1, 12 samples (48%) had no dye penetration (Grade 0)while in Group 2, 6 samples (24%) demonstrated Grade 0. Similarly, Group 2 had the most extensive dye penetration (Grade 3) in 8 of 25 samples (32%). On the other hand, Group 1 had only 2 of 25 samples (8%) in the Grade ‘3’ category [Table/Fig-1]. On comparison of the microleakage scores of the groups, a statistically significant difference was found between the two groups with a p-value<0.05 indicating a much better performance of Clinpro as compared to Helioseal F [Table/Fig-2]. Representative tooth sections for Grade 0, Grade1, Grade 2 and Grade 3 have been shown in [Table/Fig-3a-3d].
Microleakage grade for the Clinpro and Helioseal F groups (n=25) for each group.
| Grade | Group | Total | p-value |
|---|
| I – Clinpro | II – Helioseal F | Count | % |
|---|
| Count | % | Count | % |
|---|
| 0 | 12 | 48 | 6 | 24 | 18 | 36 | 0.014* |
| 1 | 7 | 28 | 5 | 20 | 12 | 24 |
| 2 | 4 | 16 | 6 | 24 | 10 | 20 |
| 3 | 2 | 8 | 8 | 32 | 10 | 20 |
| Total | 25 | 100 | 25 | 100 | 50 | 100 |
*p<0.05, Statistically significant, Chi Square test
Non parametric test - Mann Whitney test for the intergroup comparison of microleakage scores between the Clinpro and Helioseal F sealant groups.
| S. No | Group | Material | N | Mean Rank | Sum of Rank | p-value |
|---|
| 1. | I | Clinpro Group | 25 | 20.74 | 756.50 | 0.016* |
| 2. | II | Helioseal F Group | 25 | 36.26 | 518.50 |
| Total | 50 |
*p<0.05, Statistically significant, Mann Whitney U test.
The sectioned tooth samples were examined under an Optical Stereomicroscope (Carl Zeiss Stereo discovery V8, Germany). Microleakage grade scores a) Grade 0; b) Grade 1; c) Grade 2; d) Grade 3.
Discussion
Several published reports demonstrate statistically significant correlation between retention of sealant and absence of caries [14,15]. The sealants provide a physical barrier preventing the colonization of cariogenic microorganisms thereby preventing caries. The effectiveness of pit and fissure sealants depends on various conventional factors such as microleakage, penetration coefficient, tensile bond strength, viscosity of the sealant, length of resin tag formed [16]. A number of local factors influence sealant penetration into pits and fissures irrespective of the nature and type of sealant. There are several entities identified as possible contaminants of the tooth surface which include salivary pellicle, carbohydrate metabolism end products and airotor handpiece lubricating oil. The presence of such contaminants blocks the natural porosity of enamel and sealant union, which makes it necessary to do a prophylaxis before sealant application. This is also important for inhibition of marginal leakage. In the present study, maxillary and mandibular premolars extracted for orthodontic purpose, which were free of caries, developmental defects, enamel micro fractures and discoloration were included. In the present study, artificial saliva was used as a storage solution for extracted teeth, as it has no effect on the protein structure and neither does it alter the enamel structure [17]. Pumice slurry with a rubber cup was used for prophylaxis of the occlusal surfaces of premolars prior to etching. Blackwood JA et al., showed that between enameloplasty, air abrasion and pumice prophylaxis, the least microleakage was seen with the conventional pumice prophylaxis [18]. Both the materials used in the present study were applied without enameloplasty in order to observe the behavior of these materials without removal of tooth substance, as done in the in vitro study by Prabhakar AR et al., [17]. Dental materials in the oral cavity are constantly exposed to heat and pH changes [19–21] leading to formation of marginal gaps by thermal stress and microleakage stems by the different thermal expansion coefficient of tooth material and resin [22]. The coefficients of thermal expansion of resin materials (25-60 ppm/°C) are greater than that of enamel (11.4 ppm/°C) and dentin (8 ppm/°C) [23]. Therefore, to assess the in vitro performance of resin materials, thermocycling is one of the commonly used methods to simulate the long-term stresses to which the restorations are exposed [23]. In this study, the temperature range was between 5°C and 55°C, which were claimed by various studies done by Penugonda et al., and Styner D et al., to be most clinically relevant [24,25]. The evaluation of marginal integrity of the sealants by use of dyes is known to be a useful technique and used in several studies [26,27]. In the present study, a similar qualitative technique of dye penetration was used to evaluate the microleakage in the two tested sealant groups. Penetration of a dye can indicate the lack of a perfect seal but the use of different testing substances or dyes makes comparison between studies difficult. The results of the present study showed 12 of 25 samples (48%) had no dye penetration (Grade 0) in Group I (Clinpro sealant), while only 6 of 25 samples (24%) were Grade 0 in Group II (Helioseal F sealant). This result is in accordance with those obtained by Koyuturk AE et al., who reported that in thermocycling group, Helioseal F showed the highest microleakage, while Clinpro showed minimal microleakage (p<0.05) [28]. In the present study minimal microleakage was obtained in Clinpro group as compared to the Helioseal F group, this could be attributed to the lesser filler loading of 6% in Clinpro fissure sealant when compared to filler loading as high as 43% in Helioseal F fissure sealant. Lesser filler loading contributes to low viscosity which enables better penetrability into pits and fissures. Salama FS et al., evaluated the marginal seal of sealant and compomer material and concluded that the sealants penetration to the complete extent of the fissure depth is not practically possible owing to the complex fissure anatomy. Moreover, there can exist lateral fissure originating from the main fissure may not be sealed completely [29].
Clinical Implications: Pit and fissure sealants are used for the prevention of dental caries in vulnerable anatomic areas such as developmental grooves and deep occlusal fissures. The clinician should choose a material bearing in mind the ideal mechanical properties such as bond strength and minimal microleakage which could translate into maximum clinical efficacy for pediatric patients. Hence, in-vitro studies play a pivotal role in enriching the clinician on the physical properties of the materials that they use in the day to day practice.
Limitation
The limitation of this study is that teeth were restored with sealants in an environment devoid of saliva contamination and hence, further in-vivo studies are warranted.
Conclusion
The authors of the present study conclude that both the sealants used in this study showed some degree of microleakage. The least microleakage was seen with Clinpro sealant and can be a better material of choice to be used in day to day clinical practice. The present study was conducted in an in-vitro environment; care was taken to replicate the oral conditions in terms of thermocycling.
*p<0.05, Statistically significant, Chi Square test
*p<0.05, Statistically significant, Mann Whitney U test.