Meyer’s Muscle Pedicle Bone Graft a Novel Procedure in Treatment of Neglected Fracture Neck of Femur in Pediatric Age Group-A Case Report
Manjunath S Daragad1, KM Ponnanna2, Sunil Mannual3
1 Associate Professor and Consultant Deformity Surgeon, Department of Orthopaedics, SDM College of Medical Sciences and Hospital, Sattur, Dharwad, Karnataka, India.
2 Senior Resident, Department of Orthopaedics, SDM College of Medical Sciences and Hospital, Sattur, Dharwad, Karnataka, India.
3 Assistant Professor, Department of Orthopaedics, SDM College of Medical Sciences and Hospital, Sattur, Dharwad, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Manjunath S Daragad, Associate Professor and Consultant Deformity Surgeon, Department of Orthopaedics, SDM College of Medical Sciences and Hospital, Sattur, Dharwad-580009, Karnataka, India.
E-mail: daragad.manjunath@gmail.com
Meyers muscle pedicle graft has been used in delayed presentation and non-union of neck femur fracture in adults with good results. Delayed presentation or non-union neck femur in children is not uncommon in children. Subtrochanteric valgus osteotomy with or without fixation has been suggested with varying results. We present meyers muscle graft being used in paediatric age group with excellent result at 3 years follow-up. There are limited report literature of meyers muscle pedicle graft being used in children.
Harris hip score, Subtrochanteric valgus osteotomy, Trendelenberg test
Case Report
A 10-year-old girl presented to the Department of Orthopedics of SDM College of Medical Sciences and Hospital Dharwad, with history of trauma (fall from bicycle) associated with pain in the left hip and inability to bear weight on the left lower limb since 4 months. The child was taken to a local osteopath following the injury and bone tie was applied for 3 months from left hip joint extending up to the knee joint. Clinical examination revealed true shortening of 3cm associated with flexion, adduction and external rotation of hip. Assisted Trendelenberg test was positive. Hip movements were painful and restricted. Bryants triangle showed supra trochanteric shortening of 3 cm.
Investigations
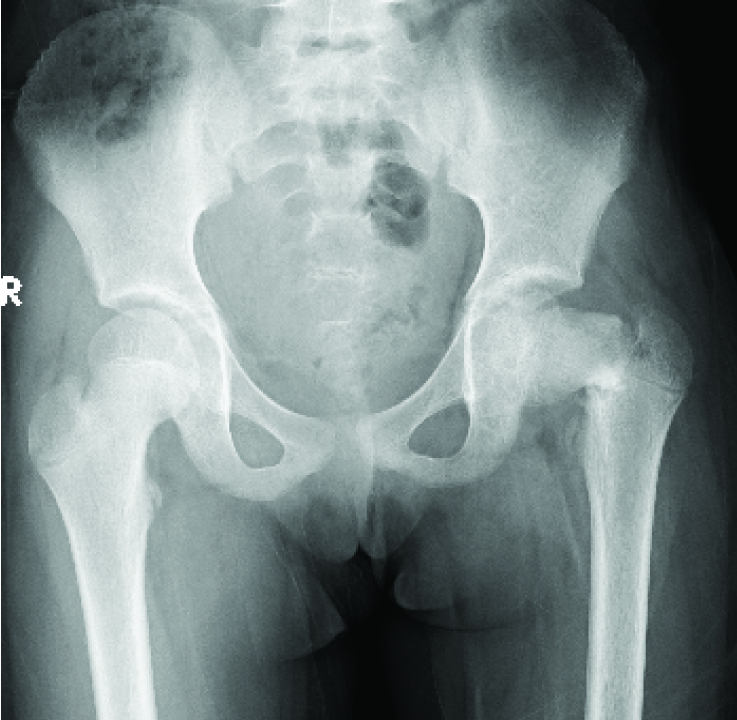
Radiograph: Showed non-union cervicotrochanteric fracture neck of left femur (Delbet type III) with varus deformity of 90° [Table/Fig-1].
Pre-operative radiograph basal neck fracture.
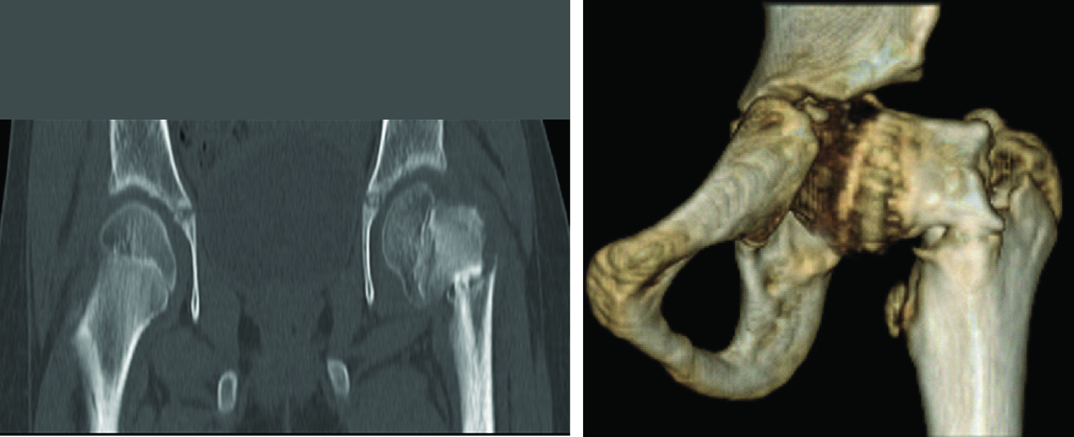
CT-scan: Revealed fracture neck of left femur with non-union, with sclerosis of the fracture ends [Table/Fig-2a,b].
CT-scan showing non-union with varus deformity.
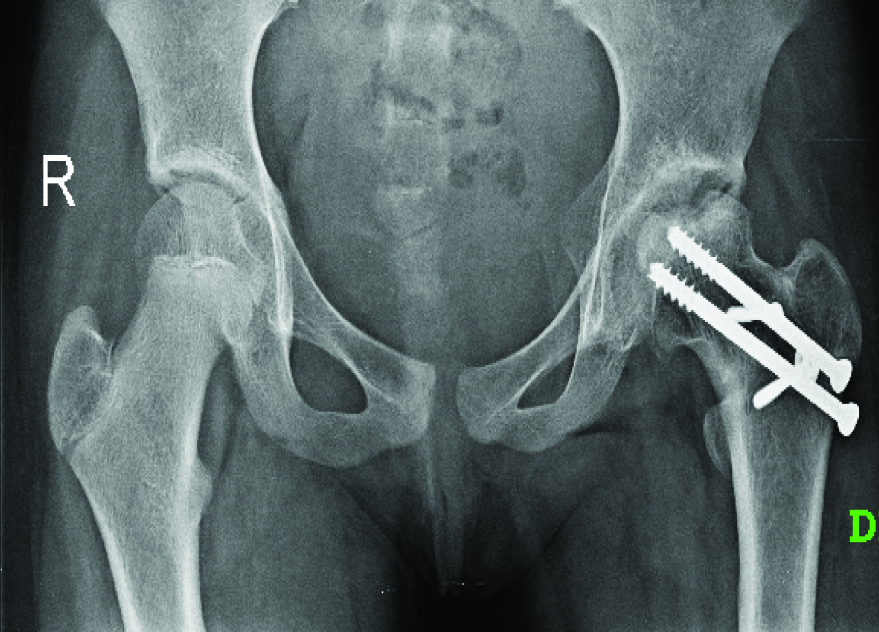
Procedure: Under spinal anaesthesia, child was put on prone position on fracture table and through posterior approach fracture site was exposed. Intraoperatively, we noted sclerosis of the fracture, which was freshened. Fracture was reduced, neck shaft angle was corrected and fixed with two 6.5mm cannulated cancellous screws. The fixation was augmented with quadratus femoris muscle which was elevated with a bone pedicle of length 4cm, width 1.5 cm and depth 1cm from its insertion on the posterior aspect of the femur. The muscle pedicle bone graft was rotated and placed posteriorly over the fracture site and pegged into the trough created in the head and fixed with two 4mm cannulated cancellous screw in posterior to anterior direction [Table/Fig-3a,b]. Wound was closed in layers over a suction drain.
a) Postoperative radiograph; b) lateral view showing graft placement. c) Four months follow-up Ratliff type II AVN.

Postoperatively: Quadriceps exercises, knee and ankle exercises were started immediately on 2nd postoperative day. Child was kept non-weight bearing for 3 months.
At 3 months follow-up there was pain relief and hip range of movements were improved and child was able to sit cross legged. At 4 months follow-up child complained of pricking sensation in the left hip. Radiograph of left hip showed Ratliff type II AVN changes- localised to the anterosuperior aspect of the femoral head [Table/Fig-3c]. The child was advised non-weight bearing mobilization and analgesics were given, following which the pricking sensation gradually subsided. At 9 months follow-up AVN changes resolved. Remodelling was seen at fracture site and union was evident [Table/Fig-4]. Child had no complaints of pricking sensation in the left hip and was comfortably carrying out her activities of daily living.
Nine month follow-up sound union and remodelling of Type II AVN.
At 36 month follow-up, the fracture showed solid union [Table/Fig-5a]. The patient had normal hip functions and was able to perform all activities of daily living like squatting, sitting cross legged and running. Harris hip score was 98 (excellent outcome) [Table/Fig-5b,c].
a) United fracture and remodelling of AVN. b) c). Functional outcome at final follow-up.

Discussion
Pediatric hip fractures are rare, accounting for less than 1% of pediatric fractures [1,2]. The vast majority of hip fractures in children, 80% to 90% are due to high energy trauma, the rest are due to moderate trauma or pathologic conditions [3]. Paediatric hip fractures are classified according to Delbet classification which has a descriptive as well as prognostic significance [4].
Cervico trochanteric fracture through base of femoral neck, second most common type of hip fracture, accounts for 25% to 30% [5–7]. According to Delbet classification the risk of AVN is 100% for transepiphyseal fracture, 50% in transcervical, 25% to 30% in cervicotrochanteric and less than 10% in Intertrochanteric fracture [3]. Delayed presentation of neck fractures is rare, but we do get neglected neck fractures in our clinical practice, mainly due to poor socio-economic status and inadequate medical treatment. There are however no clear guidelines in literature regarding the management of neglected neck fracture. Subtrochanteric valgus osteotomy has been recommended with varying results. Open Reduction Internal Fixation with muscle pedicle graft addresses problems of vascularity, augments healing process without disturbing proximal femur anatomy.
Meyers muscle pedicle graft has been a well recommended procedure for fracture neck nonunion and delayed presentation in adults with union rates of 95% [8]. However, there is limited reported literature of same procedure in paediatric age group as the incidence is very low. In developing country like India we do come across neglected neck fractures even in paediatric age group. The only recommended treatment for neglected neck fractures in paediatric age group is subtrochanteric Valgus osteotomy with varying results as reported by Ratliff [2]. They also noticed complications like shortening and non-union. Open reduction and internal fixation (ORIF) with Meyers muscle pedicle graft addresses the problem of vascularity, non-union and preserves the proximal femoral anatomy.
AK Gupta et al., in a clinical study of 32 patient, age of the patient varied from 14-62 years treated with open reduction and internal fixation with meyers muscle pedicle bone grafting reported union which was achieved in 89.5% cases, was followed-up for an average period of 3.4 years, with good functional results and had the ability to squatt and sit cross legged [9]. Results were based on hip ratting system given by Salvatti and Wilson. The results were excellent in 15 cases, good in 4 cases, fair in 4 cases and poor in 6 cases. Complications like avascular necrosis (n=2), transient foot drop (n=2), coxa- vara (n=1) and temporary loss of scrotal sensation (n=1) were noted in the study.
Delima DF et al., in a clinical study of 16 patients with ununited transcervical femoral fractures, age of the patient ranged from 12 to 40 years treated with open reduction and internal fixation with Meyers muscle pedicle bone grafting, reported radiological union in 13 patients [10].
Out of the 13 radiological unions, 9 united in varus with gardens alignment index less than 150 degrees. Four patients had a fixed flexion deformity of 10 degrees, 12 patients had external rotation restricted by 10 degrees. Functionally all the patients were able to squatt.
We applied the Meyers muscle pedicle graft in the index case where the age of the patient was 10years and got an excellent result according to Ratliff’s criteria [2]. The localised anterosuperior sectoral (Ratliff Type II) AVN is commonly noticed while treating such fractures, which resolves spontaneously. Ratliff in a case study of 71 neck fractures reported 7 cases of Type II AVN, 15 cases of Type I and 7 cases of Type III AVN. The similar AVN changes had been noticed in this case at fourth month, which resolved spontaneously when the child came for follow-up at ninthmonth. The functional outcome of hip at 3 years follow-up as assessed by Harris Hip score was excellent (98).
Conclusion
Meyers muscle pedicle graft in neglected fracture neck of femur in children can be a better treatment option as it addresses the problems of vascularity, augments healing process and it does not disturb the proximal femur anatomy.
[1]. Beaty JH, Fractures of the hip in childrenOrthop Clin North Am 2006 37(2):223-32. [Google Scholar]
[2]. Ratliff AH, Fractures of the neck of the femur in childrenJ Bone Joint Surgery (Br) 1962 44:528-42. [Google Scholar]
[3]. Mihran O Tachdjian, Hip Fractures In: John A. Herring, Cindy Godwin Daniel, Louis Nunes Hamilton edsTachdjian’s Pediatric Orthopaedics 2008 vol 34th edPhiladelphiaSaunders Elsevier:2609-30. [Google Scholar]
[4]. Koval KJ, Cantu RV, Fractures and Traumatic Dislocations Of The Hip In Children In: James McCarthy, Kenneth Noonan edsFractures in Children 2010 vol 27th edPhiladelphiaLippincott Williams & Wilkins:769-96. [Google Scholar]
[5]. Hughes LO, Beaty JH, Current concepts review: fractures of the head and neck of the femur in childrenJ Bone Joint Surg Am 1994 76:283-92. [Google Scholar]
[6]. Canale ST, Bourland WL, Fracture of the neck and intertrochanteric region of the femur in childrenJ Bone Joint Surg Am 1977 59:431 [Google Scholar]
[7]. Ingram AJ, Bachynski B, Fractures of the hip in children; treatment and resultsJ Bone Joint Surg Am 1953 35:867 [Google Scholar]
[8]. Meyers MH, Harvey JP, Moore TM, The muscle pedicle bone graft in the treatment of displaced fractures of the femoral neck: indications, operative technique and resultsOrthop Clin North Am 1974 5:779-92. [Google Scholar]
[9]. Gupta AK, Rastogi S, Nath R, Internal fixation and muscle pedicle bone grafting in femoral neck fracturesIndian Journal of Orthopaedics 2008 42(1):39-42. [Google Scholar]
[10]. Delima DF, Tanna DD, The quadratus femoris graft in old transcervical femoral fracturesJ Postgrad Med 1989 35(3):152-56. [Google Scholar]