Type 2 Diabetes Mellitus (T2DM) accounts for about 90% diabetic patients worldwide and India leads the world with more than 62 million diabetes in 2013 [1]. T2DM is on the way to become a pandemic disease in India [2,3]. As hyperglycaemia, obesity, dyslipidemia, physical inactivity and stress are common risk factors shared by T2DM and Coronary Artery Disease (CAD), an increase prevalence of diabetes points towards an escalating risk of CAD [4]. CAD is two to four times more common in diabetic patients as compared healthy populations [2,5]. The prevalence of CAD among diabetic subjects was 21.4%, which was much higher than 14.9% among subjects with impaired glucose tolerance and 9.1% among those with healthy population. CAD leads to more than 80% of all mortality and 75% of all hospitalizations in diabetic subjects [2]. Though there are wide ethnic and geographic variations in prevalence of T2DM and CAD, their association seems to be strong [6].
Adipokines are proteins/peptides with hormone like properties (some are cytokines), released from adipose tissue. Various adipokines like omentin-1, visfatin, leptin (a protein secreted by fat cells), tumor necrosis factor-α (TNF-α), resistin and adiponectin significantly affect obesity-related metabolic diseases by controlling fat metabolism, energy homeostasis and insulin sensitivity [7,8]. The obesity and atherosclerosis is linked by adipokines, as they influence the function of endothelial cells, arterial smooth muscle cells and macrophages in vessel walls [9–11].
VASPIN is a Visceral Adipose Tissue Derived Serine Protease Inhibitor, one of the more recently discovered adipokine. It inhibit the proteases responsible for insulin resistance and carotid plaque development and its rupture [12,13]. VASPIN has insulin sensing, anti-atherogenic and anti-inflammatory activities by inhibiting the Nuclear Factor-kappa B (NF-kB) thereby inhibiting the production of cytokines and adhesion molecules [14,15]. As these are beneficial effects of VASPIN, its level is found to be high in obese and T2DM patients as a compensatory factor to abrogate the chain of events leading to insulin resistance and atherosclerosis. But various studies showed that serum VASPIN levels were low in patients with T2DM microvascular complications than in patients without T2DM microvascular complications [16–18]. Also, VASPIN level was found to be low in T2DM patients with carotid plaque than without carotid plaque. There are very few studies addressing the role of VASPIN in pathogenesis of acute coronary syndrome (ACS) in patients with T2DM [19,20]. Therefore we hypothesize that decreased serum VASPIN act as a predictor of ACS in patients with T2DM.
Materials and Methods
Study population
This cross-sectional study was conducted in JIPMER hospital, Puducherry, India, after obtaining the approval from Institute Research Council and Institute Human Ethics Committee. A written informed consent was taken from study subjects, prior to recruitment. Forty-one T2DM patients as controls were recruited from Jan 2015 to Dec 2015 based on American Diabetes Association, 2010 criteria i.e., Symptoms and random plasma glucose concentration > 200 mg/dL or Fasting plasma glucose > 126 mg/dL or Two-hour plasma glucose > 200 mg/dL after oral glucose tolerance test. Forty one T2DM (> 18-year-old) patients with ACS including Unstable Angina (UA), Non- ST-elevation myocardial infarction (NSTEMI), ST-segment elevation myocardial infarction (STEMI) were recruited based on clinical presentation, electrocardiographic changes and elevation of cardiac enzymes (Troponin-I, Creative Kinase-Total and CK-MB) [21]. Patients with type 1 DM, chronic renal disease, liver cirrhosis, congestive heart failure, chronic lung diseases and chronic infections were excluded from the study. Sample size of 41 in each group was calculated by open epi software considering mean difference of 0.13 ng/ml and Standard Deviation (SD) of 0.24 ng/ml, 80% power and 90% confidence interval [19].
Clinical and biochemical characteristics of subjects at baseline
All subjects were screened with regard to medical history, height, weight, waist and hip circumferences and seated blood pressure were determined by the same observer. Body Mass Index (BMI) was also calculated. Fasting 5ml venous blood was collected from all subjects. Half of the serum separated was used for routine biochemistry investigations and remaining half was stored at −70°C for VASPIN analysis. Serum glucose (SG), total cholesterol (TC), triglycerides (TC), High Density Lipoprotein (HDL)-Cholesterol, Low Density Lipoprotein (LDL) -Cholesterol, Creatine Kinase (CK) -Total, Creatine Kinase -MB, urea and creatinine were assessed by enzymatic method on Beckman AU480 Biochemical Autoanalyser, Brea, CA, USA. Serum VASPIN levels were measured using a commercially available Enzyme-Linked Immunosorbent Assay (ELISA) kit (Ray Biotech) according to the manufacturer’s protocol, with the intra-assay and inter-assay Cofficient of Variation for pooled human serum of 9 and 11%, respectively.
Diagnosis of Acute Coronary Syndrome [
21]
ACS was diagnosed based on: 1) Clinical presentation: typical anginal pain at rest lasting more than 20 minutes, previously diagnosed angina that has become more frequent, longer in duration, or more easily provoked; and/or acute decompensated heart failure in a patient with known ischemic heart disease; 2) Electrocardiographic changes: ≥ 1-mm ST-segment elevation in at least 2 anatomically contiguous limb leads {aVL to III, including –Avr}, ≥ 1-mm ST-segment elevation in a precordial lead V4 through V6, ≥ 2-mm ST-segment elevation in V1 through V3, ST-segment depression by more than 0.05 mV in two or more contiguous leads, marked symmetrical T-wave inversion by more than 0.2 mV in the precordial leads, new bundle branch block, and/or sustained ventricular tachycardia; 3) Elevation of cardiac enzymes Troponin-I, CK-Total and CK-MB.
Statistical Analysis
Unless denoted otherwise, categorical data were described as percentages and continuous data were described as means±SD or median (inter-quartile range). A student’s t-test (for data that was normally distributed) or a Mann–Whitney test (for data that was not normally distributed) and v2 test (for data that were categorical variables) were used to compare between cases and controls. Correlations between serum VASPIN level and continuous variables were determined using Pearson’s correlation (for normally distributed data) or Spearman’s correlation (for non-normally distributed data). Receiver Operating Characteristic (ROC) curve was performed to investigate the value of serum VASPIN concentration in differentiating T2DM patients with or without ACS. Multivariable regression (Binary Logistics) modeling was used to examine effect of waist circumference, hip circumference, BMI, systolic blood pressure and duration of diabetes on serum VASPIN level for prediction of ACS risk among T2DM patients. A value of p < 0.05 was considered as statistically significant. All analysis were performed using software package SPSS 12.0 for Windows 10.
Results
Baseline clinical characteristics and biochemical measurements
Demographic, clinical and biochemical data for the (T2DM with ACS) cases and (T2DM without ACS) controls are shown in [Table/Fig-1]. The cases had a male predominance over the control group. Out of 41 ACS patients, 7 had UA, 9 had NSTEMI and 25 had STEMI. The cases had lower weight, more alcoholics and had longer duration of diabetes as compared to controls. The cases had high waist circumference, hip circumference, systolic and diastolic blood pressure and serum HDL-cholesterol and low VLDL-cholesterol and waist-hip ratio as compared to controls. The cases had normal liver and renal functions.
Clinical and Biochemical properties of the study population.
| Characteristic | Type 2 Diabetes Mellitus (T2DM) (Control) | Type 2 Diabetes mellitus (T2DM) with acute coronary syndrome (ACS)(Cases) | p-value |
|---|
| Number of patients | 41 | 41 | |
| Age (yrs) | 47.30±11.03 | 60.00±10.28 | 0.001 |
| Male/ Female | 24/17 | 33/08 | 0.03 |
| Weight (Kg) | 60.04±3.15 | 57.75±5.47 | 0.02 |
| Height (cm) | 161.86±6.40 | 163.71±7.22 | 0.22 |
| Waist circumference (cm) | 82.60±3.73 | 97.39±3.63 | 0.0001 |
| Hip Circumference (cm) | 87.32±3.83 | 107.30±3.86 | 0.0001 |
| Waist- Hip ratio | 0.94±0.01 | 0.90±0.03 | 0.0001 |
| Body mass Index (BMI) | 22.97±2.10 | 21.89±3.09 | 0.07 |
| Systolic blood pressure (mm of Hg) | 122.32±6.40 | 149.75±14.40 | 0.0001 |
| Diastolic blood pressure (mm of Hg) | 79.19±5.34 | 90.00±10.48 | 0.0001 |
| Duration of Diabetes (yrs) | 1.72±0.73 | 4.30±2.12 | 0.0001 |
| History of smoking, N (%) | 14(34.14%) | 13 (31.70%) | 0.81 |
| History of alcohol, N (%) | 7 (17.07%) | 29 (70.7%) | 0.0001 |
| Fasting plasma glucose (mg/dl) | 183.91±72.91 | 174.03±51.45 | 0.48 |
| Total Cholesterol (mg/dl) | 183.93±39.99 | 187.83±50.88 | 0.70 |
| Triglyceride (mg/dl) | 139.12±82.98 | 111.68±31.17 | 0.05 |
| HDL-C (mg/dl) | 37.74±10.37 | 44.96±11.15 | 0.01 |
| LDL-C (mg/dl) | 117.95±34.60 | 118.68±46.14 | 0.93 |
| VLDL-C (mg/dl) | 27.80±15.65 | 22.37±6.33 | 0.04 |
| CK-Total (U/L) | 127.86±51.62 | 412.93±249.04 | 0.0001 |
| CK-MB (U/L) | 15.16±5.90 | 89.25±26.70 | 0.0001 |
| Urea (mg/dl) | 23.54±6.84 | 27.90±6.41 | 0.004 |
| Creatinine (mg/dl) | 0.84±0.15 | 0.90±0.13 | 0.06 |
| Vaspin (pg/ml) | 0.83±0.29 | 0.43±0.22 | 0.0001 |
Continuous variables were described as mean±SD; categorical variables were presented as frequencies. HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; VLDL-C, very low-density lipoprotein cholesterol; CK-total, creatine Kinase-total; CK-MB, creatine kinase-MB
Serum vaspin concentration in groups
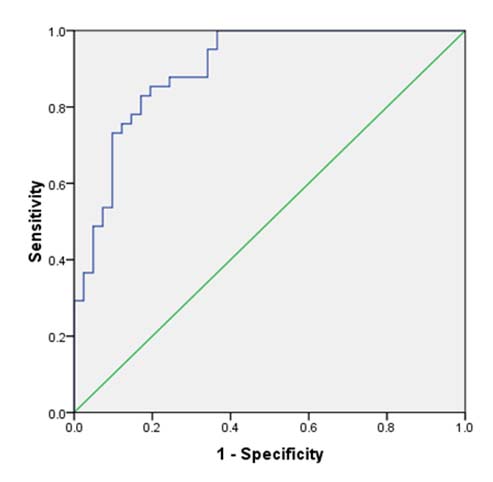
Fasting serum VASPIN concentration was lower in the cases (0.43±0.22 pg/mL) than in the controls (0.83±0.29 pg/mL) and the difference was statistically highly significant (p = 0.0001). Patients with UA (0.47±0.09 pg/mL) had higher fasting serum VASPIN level as compared to NSTEMI (0.44±0.26 pg/mL) and STEMI (0.42±0.23 pg/mL) patients, but the difference was not statistically significant. Utilizing ROC curve [Table/Fig-2] for values of VASPIN and risk of ACS among T2DM patients, it was seen that the greatest increase in risk of ACS was seen at serum VASPIN level < 0.594 pg/mL. (AUC = 0.901, sensitivity of 85% and specificity of 80%, LR = 4.25, p< 0.0001).
Receiver Operating Characteristic (ROC) curve confirmed that serum vaspin concentration significantly differentiated type 2 diabetes mellitus patients with or without acute coronary syndrome, AUC = 0.901, p < 0.001 for significant AUC.
Correlation between serum vaspin concentration and clinical parameters
Correlation analysis undertaken on all T2DM patients showed serum VASPIN concentration was negatively correlated with age, waist circumference, hip circumference, systolic and diastolic blood pressure, duration of diabetes, serum CK-Total, CK-MB and urea levels [Table/Fig-3]. Multivariate regression (Binary logistics) analysis after adjusted for waist circumference, hip circumference, BMI, systolic blood pressure and duration of diabetes showed that serum VASPIN was not significantly associated with ACS risk among T2DM patients{OR: 3.50, Adjusted OR (95%CI): 32.85 (7.04 – 153.52)}.
Correlation between vaspin and other variables among study population.
| Parameter | Type 2 Diabetes Mellitus patients TOTAL (N= 82) | Type 2 Diabetes Mellitus patients without acute coronary syndrome (Control, N= 41) | Type 2 Diabetes mellitus patients with acute coronary syndrome (Cases, N=41) |
|---|
| r values | p-value | r values | p-value | r values | p-value |
|---|
| Age | -0.294 | 0.007 | 0.038 | 0.813 | 0.008 | 0.960 |
| Weight | 0.189 | 0.089 | -0.103 | 0.522 | 0.150 | 0.349 |
| Height | -0.104 | 0.352 | -0.031 | 0.847 | -0.033 | 0.838 |
| Waist circumference | -0.575 | 0.0001 | -0.146 | 0.362 | 0.066 | 0.682 |
| Hip Circumference | -0.569 | 0.0001 | -0.146 | 0.362 | 0.294 | 0.062 |
| Waist- Hip ratio | 0.315 | 0.003 | 0.122 | 0.447 | -0.152 | 0.343 |
| Body mass Index | 0.156 | 0.161 | -0.007 | 0.965 | 0.112 | 0.485 |
| Systolic blood pressure | -0.433 | 0.0001 | 0.077 | 0.632 | 0.131 | 0.414 |
| Diastolic blood pressure | -0.276 | 0.012 | 0.251 | 0.113 | -0.003 | 0.985 |
| Duration of Diabetes | -0.399 | 0.001 | -0.182 | 0.254 | 0.055 | 0.733 |
| Fasting plasma glucose | 0.112 | 0.316 | -0.073 | 0.650 | -0.039 | 0.809 |
| Total Cholesterol | - 0.099 | 0.376 | -0.172 | 0.282 | -0.025 | 0.877 |
| Triglyceride | 0.120 | 0.282 | 0.013 | 0.935 | -0.077 | 0.632 |
| HDL-C | -0.191 | 0.085 | 0.112 | 0.485 | -0.127 | 0.429 |
| LDL-C | -0.075 | 0.503 | -0.248 | 0.118 | 0.047 | 0.770 |
| VLDL-C | 0.115 | 0.303 | 0.010 | 0.950 | -0.086 | 0.593 |
| CK-Total | - 0.475 | 0.0001 | -0.378 | 0.014 | -0.143 | 0.372 |
| CK-MB | -0.407 | 0.0001 | 0.008 | 0.960 | -0.020 | 0.901 |
| Urea | -0.299 | 0.006 | -0.268 | 0.090 | 0.012 | 0.940 |
| Creatinine | -0.142 | 0.203 | -0.136 | 0.340 | 0.133 | 0.407 |
HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; VLDL-C, very low-density lipoprotein cholesterol; CK-total, creatine Kinase-total; CK-MB, creatine kinase-MB
Discussion
The present study was carried out to see the association between serum VASPIN level and risk of ACS in T2DM patients. Eighty two T2DM patients were recruited for the study. Out of 82 patients, 41 T2DM patients had ACS. Out of 41 T2DM patients with ACS, 7 were UA, 9 were NSTEMI and 25 were STEMI. In the present study, there were significant differences between T2DM patients with ACS and T2DM patients without ACS with respect to risk factors like alcohol, blood pressure and duration of diabetes. There were no significant differences between them with regards to other conventional risk factors like BMI, hyperlipidemia and smoking.
In the current study, correlation analysis among all T2DM patients (cases and controls) showed that serum VASPIN concentration was negatively correlated with age, waist circumference, hip circumference, systolic and diastolic blood pressure, duration of diabetes, serum CK-Total, CK-MB and urea. Tan et al., found higher serum and adipose tissue VASPIN levels in women with Polycystic Ovarian Syndrome (PCOS) and detected significant positive associations between circulating VASPIN and VASPIN levels in omental adipose tissue with BMI and waist-to-hip ratios [22]. Jian W et al., showed that the serum VASPIN concentration was significantly correlated with body mass index, Waist-Hip Ratio (WHR) and homeostasis model assessment of insulin resistance in T2DM patients [23].
The increase in VASPIN may be a compensatory response to antagonize the action of other unknown proteases that are up-regulated in obesity and in states of insulin resistance; hence, this up-regulation may be a defensive mechanism against insulin resistance [24]. In our study, fasting serum VASPIN level was significantly lower among T2DM patients with ACS as compared to T2DM patients without ACS, thus suggesting that VASPIN may have anti-atherosclerotic and anti-inflammatory properties. The serum concentration of VASPIN may, therefore, be associated with the process of carotid and coronary plaque development in the early stage and plaque rupture in late stage of T2DM [12,14,25]. Jung CH et al., showed that the anti-atherogenic role of VASPIN is due to attenuation of cytokine induced gene expression of adhesion molecules by inhibiting NF-kB following Adenosine monophosphate-activated protein kinase (AMPK) activation [26]. Similar observations were shown by other studies that suggested that the measurement of serum VASPIN may be used for assessing the risk of ACS among T2DM patients. Utilizing ROC curve for values of VASPIN and risk of ACS among T2DM patients, it was seen that the greatest increase in risk of ACS was seen at fasting serum VASPIN level of < 0.594 pg/ml.
Our data showed that T2DM patients with lower serum VASPIN level had lower body weight, longer duration of diabetes and presence of ACS. Various studies [17,19] have showed that serum VASPIN level is low in patients with reduced body weight, longer duration of diabetes and occurrence of complications. Lower serum VASPIN level was observed not only with development of ACS but also in other micro-vascular complications. Gulcelik et al., showed that T2DM patients with neuropathy, retinopathy and nephropathy had lower serum vaspin concentration than in patients without these complications [16]. VASPIN has an anti-apoptotic effect in endothelial cell [27,28] and anti-inflammatory and anti-migratory effects in vascular smooth muscle cell [25,26].
Limitation
The limitations of the study were that the control subjects were not normal people, but outpatients with T2DM. This inclusion method cannot exclude some confounding effects, including the effects of disease itself and drugs treatment. Non-recruitment of newly diagnosed T2DM patients, the different duration of disease and different treatment in each patient may incorporate a possible source of selection bias. The study population was relatively small; however, the study has sufficient power to detect the influence of serum VASPIN levels on risk of ACS among T2DM patients. This was a cross-sectional study, and thus it was difficult to evaluate a cause-effect relationship between serum vaspin levels and ACS.
Conclusion
This work represents advancement in biomedical science because it shows that low serum VASPIN concentration may be a risk factor and an independent variable for ACS in type 2 DM patients. These findings may have important implications both for understanding the pathophysiology of ACS and for the development of future therapeutic and coronary preventive approaches.
Funding: This study was funded by Intramural research grant from JIPMER, Puducherry.
Author Contributions
Aswathy JS: Study concept and design; analysis and interpretation of data.
Dr. Prashant S. Adole: Study concept and design; drafting of the manuscript; critical revision of the manuscript for important intellectual content.
Dr. Mukta Wyawahare: Study concept and design; diagnosis of controls; acquisition, analysis and interpretation of data; final approval of the version to be published.
Dr. Rama Prakasha Saya: Study concept and design; analysis and interpretation of data; drafting of the manuscript; final approval of the version to be published; critical revision of the manuscript for important intellectual content.