Introduction
Root canal preparation leads to deviation of the canal anatomy causing canal transportation which affects the success of the treatment. Cone Beam Computed Tomography (CBCT) is a non invasive imaging technique to analyse the shape of the root canal before and after the preparation.
Aim
The purpose of this study was to investigate and evaluate the canal transportation in curved mandibular molar root canals and centering ability of Reciproc and One Shape file systems after instrumentation using CBCT.
Materials and Methods
Twenty mandibular molars were taken and allocated into two groups (n=10): Group 1-One Shape and Group 2-Reciproc. The canals were then scanned using CS 3D CBCT scanner (Carestream) before and after preparation, to assess the transportation and centering values at different levels respectively from the apex. The data gathered were then assessed statistically with Mann-Whitney test.
Results
Analysis revealed that Reciproc and One Shape showed statistically no significant difference in terms of canal transportation and centering ability (p>0.05).
Conclusion
One shape and Reciproc performed similar in terms of canal transportation & centering ability.
NiTi, Shaping ability, Single file, Reciprocating, Root canal preparation
Introduction
Chemomechanical preparation is a fundamental part of the root canal therapy [1]. The cardinal goals of cleaning and shaping are thorough debridement and shaping of the root canal system, while maintaining the original canal configuration and optimal canal form [2,3] which is difficult to achieve in curved root canals.
Canal curvature is considered to be the principal risk factor for procedural errors enlisting ledges, zips, perforations and root canal transportation [4]. Cimis GM et al., observed that 46% of curved canals had varying degrees of apical transportation after instrumentation [5]. The restoring forces of the file create a tendency for the endodontic file systems to straighten the root canal that results in the canal transportation [6].
Recent research in rotary Nickel-Titanium (NiTi) instrument have led to new design formulations due to which the original canal shape is preserved leading to less iatrogenic errors [7,8]. With the quest of increasing the operator’s efficiency and decreasing the time required, single file systems were introduced.
Among the entire range of single file systems, One Shape and Reciproc have been selected for the study. Although both are single file systems yet they have been selected as One Shape uses rotating motion and Reciproc works on reciprocation.
One Shape (Micro Mega, Besancon, France) rotates in a clockwise motion for a quicker and a safer root canal preparation. Along the whole length of the file, an uneven cross-sectional pattern of the file produces the drifting wave of motion.
During shaping of the canal, rotary instruments can lead to an increased level of strain and fatigue which can cause instrument distortion or separation which is the major drawback of the NiTi rotary instruments [9]. The concept of reciprocating motion makes it possible to decrease the hazard of instrument separation [10]. The NiTi files moves in a to and fro “reciprocal motion” in a “balanced force” technique [11,12]. Reciproc (VDW, Munich, Germany) has an S-shaped cross-section and sharp cutting edges that shape the canal by means of a reciprocal back vand forward motion with 150° counter clockwise and 30° clockwise rotation. The reciprocating instrument is first moved in a cutting direction and then reverses the instrument to release. Reciproc has been prepared from M-wire technology which has an increased resistance to fatigue than the conventional NiTi alloy [8,13].
CBCT is a non invasive imaging technique used for analysis of craniofacial areas that produces more realistic images that facilitates interpretation. It becomes possible to analyse the shape of the root canal before and after the preparation by using CBCT. Thus, the objective of the present study was to assess the canal transportation in mandibular molar root canals and centering ability of One Shape and Reciproc file systems using CBCT imaging.
This study aimed at comparing the centering ability and canal transportation of One Shape and Reciproc file systems through CBCT. There is a lacuna in literature comparing the rotary and reciprocating file systems, since reciprocating file systems claim to decrease iatrogenic errors during canal preparation according to their manufacturers. The null hypothesis generated was that rotating and reciprocating motions perform similar in terms of centering ability and canal transportation.
Materials and Methods
A total of 20 extracted mandibular molar teeth (average length of 20-21mm) were collected from the Department of Oral and Maxillofacial Surgery, Inderprastha Dental College, Sahibabad for the present in vitro study. The inclusion criteria were fully formed root apices with mesiobuccal canal curvature (20-35°) according to Schneider’s method [14]. The distal roots were discarded after sectioning them at the furcation level. Previous literature confirms of more curvature and iatrogenic errors in mesial canals of mandibular molars, thus mesial canals were selected. The teeth with immature open root apices, calcified canals, apical resorption and anatomic variations were excluded from the study. The teeth were then disinfected and stored in 10% formalin solution.
Using an Endo Access bur (Dentsply, Maillefer) the access cavities were prepared and the mesiobuccal canals were located. The patency was then achieved using #10K-file.
In Group 1, the One Shape system was used till the working length of each canal with the Marathon (Saeyang) Endo A class endomotor set to 350 rpm and 3 N cm torque with a 16:1 contrangle. It is a single endodontic file with variable pitch and a pilot tip having a tip diameter 0.25 mm and 0.06 taper.
In Group 2, the Reciproc instrument was moved in a slow in and out pecking motion till the working length. R25 file with 0.25 mm of diameter and a taper of 8% were used to prepare the canal. The reciprocating motor X-Smart Plus (Dentsply, Maillefer) was used.
A 5.25% NaOCl was used for irrigation after usage of the files in both the groups. Removal of smear layer was performed by using 17% EDTA for one minute. The teeth were then scanned based on the parameters using CBCT imaging. The data collected was then evaluated using SPSS software statistical analysis.
Post Instrumentation Scans
Using the same protocol and settings as for the preinstrumented scans, all prepared canals were scanned using CBCT. All CBCT images were assessed utilizing the on demand software for CS 3D, Carestream Dental CBCT system.
Assessment of the Root Canal Preparation
Canal transportation was assessed by measuring the shortest distance from the edge of uninstrumented canal to the periphery of the root (mesial and distal). These readings were compared with the same measurements obtained from the instrumented images.
The canal transportation was calculated by using Gambill JM et al., formula which is (a1-a2)-(b1-b2), here a1 is the distance from the mesial wall of the unprepared canal root to the unprepared wall, b1 is the distance from distal wall of the unprepared canal to the distal wall of the root, a2 is the distance from mesial wall of the prepared canal to the the mesial wall of the root, and b2 is the distance from distal wall of the prepared canal root to the distal wall of the root [15]. [Table/Fig-1] clarifies the notations. A result other than 0 specifies that transportation has occurred in the canal.
Measurement for image cross-section with the notations.
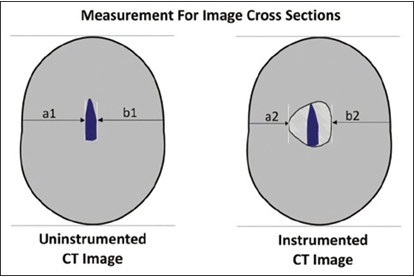
The mean centering ratio demonstrates the ability of the instrument to stay centered in the canal. It was calculated for each section by using the following ratio: (a1-a2)/(b1-b2) or (b1-b2)/(a1-a2). If these numbers are not equal, the lower figure calculated is considered as the numerator of the ratio. According to this formula, a result value of 1 indicates perfect centering [15].
Results
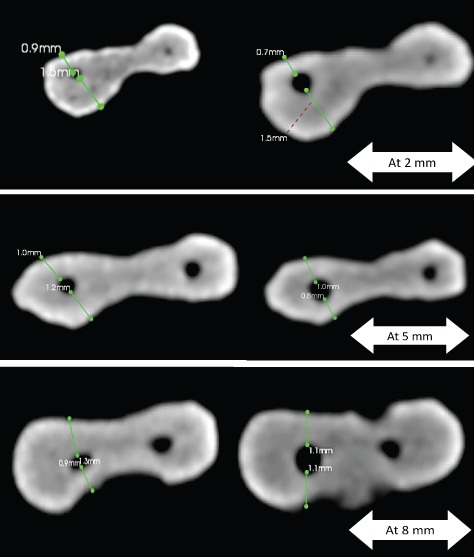
[Table/Fig-2] shows pre and post instrumentation representations of CBCT scans at selected levels of 2 mm, 5 mm and 8 mm from the apex.
Pre and Post instrumentation CBCT scans at levels 2 mm, 5 mm and 8 mm.
The mean and standard deviation values for canal transportation and the centering ratio after instrumentation are presented in [Table/Fig-3,4].
The mean and standard deviation values of canal transportation after instrumentation at 2 mm, 5 mm and 8 mm [1].
| Levels | Groups | Mean±SD | Median | p-value |
|---|
| 2 mm | One Shape | 0.48±1.31 | 0 | 0.28 |
| Reciproc | 0.2±0.141 | 0.1 |
| 5 mm | One Shape | 1.2±1.15 | 1.9 | 0.131 |
| Reciproc | 2.08±0.164 | 2.2 |
| 8 mm | One Shape | 0.50±1.46 | 0 | 0.73 |
| Reciproc | 1.92±0.46 | 1.8 |
Mann-Whitney test
The mean and standard deviation values of centering ability after instrumentation at 2 mm, 5 mm and 8 mm [1].
| Levels | Groups | Mean ± SD | Median | p-value |
|---|
| 2 mm | One Shape | 0.38±0.32 | 0 | 0.184 |
| Reciproc | 0.72±0.40 | 1 |
| 5 mm | One Shape | 0.40±0.15 | 0.1 | 0.209 |
| Reciproc | 0.32±0.43 | 0 |
| 8 mm | One Shape | 0.6±0.13 | 0 | 0.242 |
| Reciproc | 0.18±0.16 | 0.3 |
Mann-Whitney test
At 2 mm, Reciproc showed lower mean canal transportation (0.20±0.14) & higher centering ability (0.72±0.40) as compared to One Shape, whereas at 5 mm, Reciproc showed higher canal transportation (2.08±0.164) and lower centering ability (0.32±0.43) and at 8 mm also, Reciproc showed higher canal transportation (1.92±0.46) and lower centering ability (0.18±0.16) as compared to One Shape.
Although, Reciproc showed more canal transportation as compared to One Shape but Mann-Whitney test revealed that there was no statistically significant difference between the two single file systems (p>0.05).
Discussion
Achieving ideal cleaning and shaping of the root canal systems is very challenging. Schneider advocates a funnel shaped canal with smallest diameter at the apical constriction to be the most suitable for three dimensional fluid tight seal [1]. Most endodontic instruments during instrumentation straighten the canal leading to loss of working length.
In the present study, on assessing the canal transportation and centering ability between the One Shape and Reciproc file systems, there was no significant difference found between them. Saber SE et al., showed that Wave One and Reciproc had no significant difference in canal transportation as compared to One Shape (p>0.05) [16].
Canal curvature is suspected to be the prime risk factor for instrument failure because of flexural stresses and cyclic fatigue [8,16,17]. A continuously rotating instrument around a curve generates extension and compression forces within the file resulting in flexural fatigue, which results in instrument separation [18]. Therefore, even if it is possible to try to maintain the original canal configuration and optimal form while shaping [2], the stresses on the files cannot be reduced.
Single file systems are an evolution towards simplicity, as compared to multiple file systems.
Single file systems save the operator’s time, cost and reduce the chances of cross contamination between patients. It also reduces instrument fatigue hence prevent instrument separation in the canal- a fear every dentist lives in. NiTi single file systems are classified in terms of the motion as continuous rotary and reciprocating motion. One Shape and F360 are examples of single file continuous rotary motion whereas WaveOne and Reciproc are examples of single file reciprocating motion [19]. In this study, we have used One Shape and Reciproc single file systems.
The fifth generation of NiTi files has a wave like pattern of motion along the length of the file while rotating due to the offset center of mass and/or the center of rotation. The wave like motion causes the file to engage and disengage along the canal wall which reduces the stresses produced between the file and the canal wall [20].
One Shape rotary NiTi files (MicroMega) is manufactured from austenite 55-NiTi alloy. It has three different cross-section zones; the coronal portion of the file is provided with two cutting edges, the middle portion of the file has a cross-section that progressively changes from two to three cutting edges and the apical portion of the file present a variable three cutting edge design [21].
Reciprocating motion causes the instrument to move in clockwise direction for cutting first and then in anticlockwise direction to release the instrument making a complete circle of 360 degrees. The clockwise motion is greater than anticlockwise motion and the instrument progresses towards the apex [22]. Reciproc files are manufactured by M wire technology. This technology makes the endodontic files different from conventional file systems as it increases the flexibility and fatigue resistance of the files. This study shows that comparable value of mean canal transportation and centering ability of Reciproc with that of One Shape which is statistically insignificant, although the little difference might be due to a new M wire technology used for manufacturing Reciproc instrument.
There have been no studies comparing these two file systems so far, but several studies have compared the two motions. One such study showed that the differences between One Shape (rotary) and Wave One (reciprocating) was not statistically significant [23]. There have been contradictory results as well. A study concluded that Wave One showed lesser transportation and better centering ability than One Shape and ProTaper [24].
This study being an in vitro analysis is limited as clinical scenario is different, hence further in vivo studies can be undertaken to substantiate the results of this study in vivo condition.
Conclusion
Within the limitation of this study, both the tested files performed similar with no statistically significant difference in terms of canal transportation and centering ability (p>0.05).
However, further investigations are needed to evaluate and authenticate the results of this study in terms of canal transportation and centering ability between the two file systems.
Mann-Whitney test
Mann-Whitney test
[1]. Schilder H, Cleaning and shaping the root canalDent Clin North Am 1974 18:269-96. [Google Scholar]
[2]. Arora A, Taneja S, Kumar M, Comparative evaluation of shaping ability of different rotary NiTi instruments in curved canals using CBCTJ Conserv Dent 2014 17(1):35-39. [Google Scholar]
[3]. Uzunoglu E, Turker SA, Comparison of canal transportation, centering ratio by cone-beam computed tomography after preparation with different file systemsJ Contemp Dent Pract 2015 16(5):360-65. [Google Scholar]
[4]. Weine FS, Kelly RF, Lio PJ, The effect of preparation procedures on original canal shape and on apical foramen shapeJ Endod 1975 1(8):255-62. [Google Scholar]
[5]. Cimis GM, Boyer TJ, Pelleu GB, Effect of three file types on the apical preparation in moderately curved canalsJ Endod 1988 14:441-44. [Google Scholar]
[6]. Bender IB, Freeland JB, Clinical considerations in the diagnosis and treatment of intra-alveolar root fracturesJ Am Dent Assoc 1983 107(4):595-600. [Google Scholar]
[7]. Gambarini G, The K3 rotary nickel titanium instruments systemEndod Topics 2005 10:179-82. [Google Scholar]
[8]. Peter OA, Current challenges and concepts in the preparation of root canal systems: A reviewJ Endod 2004 30(8):559-67. [Google Scholar]
[9]. Câmara AC, Aguiar CM, Figueiredo JAP de, Assessment of the deviation after biomechanical preparation of the coronal, middle, and apical thirds of root canals instrumented with three Hero rotary systemsJ Endod 2007 33:1460-63. [Google Scholar]
[10]. Kandaswamy D, Venkateshbabu N, Porkodi I, Pradeep G, Canal-centering ability: An endodontic challengeJ Conserv Dent 2013 12:3-9. [Google Scholar]
[11]. Johnson E, Lloyd A, Kuttler S, Namerow K, Comparison between a novel nickel-titanium alloy and 508 nitinol on the cyclic fatigue life of ProFile25/.04 rotary instrumentsJ Endod 2008 34:1406-09. [Google Scholar]
[12]. Gambarini G, Advantages and disadvantages of new torque-controlled endodontic motors and low-torque NiTi rotary instrumentationAus Endod J 2001 27(3):99-104. [Google Scholar]
[13]. Gernhardt CR, One shape- a single file system for root canal instrumentation used in continuous rotationENDO(LondEngl) 2013 7:211-16. [Google Scholar]
[14]. Schneider SW, A comparison of canal preparation in straight and curved root canalsOral Surg Oral Med Oral Pathol 1971 32:271-75. [Google Scholar]
[15]. Gambill JM, Alder M, del Rio CE, Comparison of nickel-titanium and stainless steel hand-file instrumentation using computed tomographyJ Endod 1996 22:369-75. [Google Scholar]
[16]. Saber SE, Nagy MM, Schäfer E, Comparative evaluation of the shaping ability of WaveOne, Reciproc and OneShape single-file systems in severely curved root canals of extracted teethInt Endod J 2014 48(1):109-14. [Google Scholar]
[17]. Hulsmann M, Peters OA, Dummer PM, Mechanical preparation of root canals: Shaping goals, techniques and meansEndod Topics 2005 10:30-76. [Google Scholar]
[18]. Capar ID, Ertas H, Ok E, Arslan H, Ertas ET, Comparative study of different novel nickel-titanium rotary systems for root canal preparation in severely curved root canalsJ Endod 2014 40:852-56. [Google Scholar]
[19]. Kumar SR, Gade V, Single file niti-rotary systemsInt J Med and Dent Sci 2015 4(1):701-07. [Google Scholar]
[20]. Hashem AA, Ghoneim AG, Lutfy RA, Foda MY, Omar GA, Geometric analysis of root canals prepared by four rotary NiTi shaping systemsJ Endod 2012 38:996-1000. [Google Scholar]
[21]. Karova E, Topalova-Pirinska S, Waveone and one shape files: Survival in severely curved artificial canalsGlobal Journal of Medicine Research 2014 14(4):1 [Google Scholar]
[22]. Burklein S, Tsotsis P, Schafer E, Incidence of dentinal defects after root canal preparation: Reciprocating versus rotary instrumentationJ Endod 2013 39(4):501-04. [Google Scholar]
[23]. Agarwal RS, Agarwal J, Jain P, Chandra A, Comparative analysis of canal centering ability of different single file systems using cone beam computed tomography- An in vitro studyJ Clin Diagn Res 2015 9(5):ZC06-ZC10. [Google Scholar]
[24]. Tambe VH, Nagmode PS, Abraham S, Patait M, Lahoti PV, Jaju N, Comparison of canal transportation and centering ability of rotary protaper, one shape system and wave one system using cone beam computed tomography: An in vitro studyJ Conserv Dent 2014 17(6):561-65. [Google Scholar]